
Although much is known about the U.S. health disadvantage, every chapter of this report has identified gaps in the evidence for documenting its scope, understanding its causes, and identifying effective solutions. It is clear that further research in epidemiology, demography, health services, economics, and political science is necessary to fully understand the root causes of the U.S. health disadvantage. The specific deficiencies in each topic area are too extensive to summarize here, and the literature in each field often includes articles that document specific research challenges. However, this report has identified several recurring themes that point to important priorities for research on cross-national differences in health.
This chapter focuses on advancing the science for understanding the U.S. health disadvantage, but we emphasize that such efforts should not come at the expense of vitally important fields of research that focus on how to reduce morbidity and mortality from today’s leading health threats, including the nine conditions responsible for the U.S. health disadvantage documented in Part I. In general, cross-national comparisons provide only clues as to why one population is healthier than another. Investigating these important hypotheses should not detract from research on specific diseases and injuries and on effective interventions and policies to improve health outcomes in the United States. Research in the areas of biomedicine, health services, public health, social epidemiology, and the social, behavioral, and environmental sciences are all vital. Diverting support or funding for these important research endeavors to study the U.S. health disadvantage would be a fundamental mistake.
We also emphasize that our call for more research should not be used as an excuse for inaction on the part of the nation. As detailed in Chapter 10, the causes of the U.S. health disadvantage are clear enough, and there is sufficient evidence to justify an immediate response on the part of the nation, states, and local communities. The public health and social policy priorities are evident, and interventions of proven effectiveness are known. Delaying action to wait for more data will only allow the U.S. health disadvantage to grow (see Chapter 10).
Research can point to priority areas for action, but its value will depend on the quality of available cross-national data. This chapter focuses on how to build capacity for productive scholarship on international health differences and the need for an ongoing and coordinated commitment by research agencies, funding bodies, statistical agencies, and investigators. We focus on four areas: (1) data needs, (2) analytic methods development, (3) new lines of inquiry, and (4) stable research funding.
High-income countries currently collect extensive data on health indicators and a variety of factors that contribute to health and illness. The United States is among the countries with the most extensive efforts to collect health-related data using large population-based surveys. Large nationally representative population health surveys conducted by the U.S. Department of Health and Human Services include the National Health Information Survey (NHIS), the Behavioral Risk Factor and Surveillance System (BRFSS) survey, the National Health and Nutrition Examination Survey (NHANES), and the National Ambulatory Medical Care Survey (NAMCS). The BRFSS program has been systematically collecting risk factor data in a state-based system for nearly three decades. It is one of the few worldwide examples of a sustained systematic collection of data that tracks risk factors over time at the population level. Population surveys conducted by other agencies are also relevant to this topic, including the decennial U.S. census, the American Community Survey, the Current Population Survey, and surveys conducted by the U.S. Department of Education.
Data collection efforts in other countries range from local or provincial surveys to nationally representative survey methodologies and some cooperative multinational efforts to administer similar survey instruments to comparable populations in each country. An example of the latter is the Survey of Health, Ageing and Retirement in Europe (SHARE), the English Longitudinal Study on Ageing (ELSA), and the Health and Retirement Study (HRS). For a detailed list of data sets that are available for research (see Table 9-1).
In the United States, the National Institutes of Health (NIH)—and the National Institute on Aging in particular—has played a leadership role in
| STUDY FEATURES | ||||||||
| DATABASE | Baseline Sample Size | Start Year | End Year | Longitudinal | International | Minority Oversample(s) | Anthropometric Measures | Biospecimens |
| AVAILABLE DATA SETS | ||||||||
| Advanced Cognitive Training for Independent and Vital Elderly (ACTIVE) | 2,802 | 1999 | 2011 | X | X | X | X | |
| Aging, Status, and the Sense of Control (ASOC) | 2,593 | 1995 | 2001 | X | ||||
| Alameda County Health and Ways of Living Study | 6,928 | 1965 | 1999 | X | X | |||
| Americans Changing Lives Study (ACL) | 3,617 | 1986 | Pres | X | X | |||
| Assessment of Doctor-Elderly Patient Encounters (ADEPT) | 46 | 1998 | 2001 | X | X | |||
| The Australian Longitudinal Study of Ageing (ALSA) | 2,087 | 1992 | 2010 | X | X | X | X | |
| Census Microdata Samples Project (also known as The Status of Older Persons in UNECE Countries) | ~1 million | 1989 | 1992 | X | X | |||
| The Charleston Heart Study (CHS) | 2,283 | 1960 | Pres | X | X | X | ||
| China Health and Retirement Longitudinal Study (CHARLS) | 17,000 | 2008 | Pres | X | X | X | X | |
| Chinese Longitudinal Healthy Longevity Survey (CLHLS) | 8,993 | 1998 | Pres | X | X | X | ||
| Costa Rican Longevity and Healthy Aging Study (CRELES) | 2,827 | 2004 | Pres | X | X | X | X | |
| The Cross National Equivalent Files (CNEF) | 12,900-45,000+ | 1970 | 2010 | X | X | X | X | |
| Cross-Sectional and Longitudinal Aging Study | 2,891 | 1989 | 1992 | X | X | |||
| Early Indicators of Later Work Levels, Disease, and Death (EI) | 39,338 | 1850 | 1930 | X | X | X | ||
| STUDY FEATURES | |||||||||
| DATABASE | Baseline Sample Size | Start Year | End Year | Longitudinal | International | Minority Oversample(s) | Anthropometric Measures | Biospecimens | |
| English Longitudinal Study of Ageing (ELSA) | 12,100 | 2000 | Pres | X | X | X | X | ||
| Epidemiology of Chronic Disease in the Oldest Old | 1970-1979: 2,877 1980-1988: 3,113 | 1970 | 1988 | X | X | ||||
| Established Populations for Epidemiologic Studies of the Elderly (EPESE) | 14,458 | 1981 | 1993 | X | X | X | |||
| German Socio-Economic Panel (GSOEP)—see also Cross National Equivalent Files (CNEF) above | 20,000+ | 1984 | 2011 | X | X | ||||
| Health and Retirement Study (HRS) | 22,000+ | 1992 | Pres | X | X | X | X | ||
| Health Conditions of Elderly Puerto Ricans (PREHCO) | 5,336 | 2000 | 2006 | X | X | X | X | ||
| Human Mortality Database | 37 | countries | 1751 | Pres | X | X | |||
| Indonesian Family Life Survey (IFLS) | 22,000-44,000 | 1993 | 2008 | X | X | X | X | ||
| International Database (IDB) | 226 | countries | 1950 | Pres | X | ||||
| Iowa 65+ Rural Health Study | 3,673 | 1991 | 2001 | X | X | X | |||
| Japanese Study on Aging and Retirement (JSTAR) | 4,200 | 2007 | X | ||||||
| Irish Longitudinal Study on Ageing (TILDA) | 8,000+ | 2009 | Pres | X | X | X | X | X | |
| Korean Longitudinal Study of Aging (KLoSA) | 10,000+ | 2006 | Pres | X | X | ||||
| Longitudinal Aging Study in India (LASI) | 1,500+ | 2010 | Pres | X | X | X | X | ||
| Longitudinal Employer-Household Dynamics (LEHD) | 48 | states or U.S. territories | 1991 | Pres | X | ||||
| Longitudinal Studies of Aging (LSOAs) | 1984-1990: | 7,541 1994-2000: | 9,447 1984 | 2000 | X | ||||
| Longitudinal Study of Generations | 300+ three-generation families, 2,000+ individuals | 1971 | 2001 | X | |||||
| Longitudinal Study of Mexican-American Elderly Health (The Hispanic EPESE) | 3,050 | 1993 | 2006 | X | X | X | |||
| Los Angeles Family and Neighborhood Survey (L.A.FANS) | 2,548 | 2000 | 2008 | X | X | X | X | ||
| The Luxembourg Income Study (LIS) | 30 | countries | 1968 | Pres | X | ||||
| Matlab Health and Socioeconomic Survey (MHSS) | Main survey: 4,364 households | 1996 | Pres | X | |||||
| Mexican Family Life Survey (MxFLS) | 35,000+ | 2002 | 2013 | X | X | X | X | ||
| Mexican Health and Aging Study | 15,186 | 2001 | Pres | X | X | X | X | ||
| Midlife Development in Japan (MIDJA) | 1,027 | 2008 | Pres | X | X | X | X | X | |
| Midlife Development in the United States (MIDUS) | 1995-1996: 7,108 2004-2006: 5,555 | 1995 | Pres | X | X | X | X | ||
| National Archive of Computerized Data on Aging (NACDA) | |||||||||
| National Health and Aging Trends Study (NHATS) | 8,000+ | 2011 | Pres | X | X | X | |||
| National Long Term Care Survey (NLTCS) | 20,485 | 1982 | 2004 | X | X | X | |||
| National Longitudinal Mortality Study (NLMS) | ~3.3M | 1973 | 2010 | X | |||||
| National Longitudinal Survey: 1990 Resurvey of Older Males (NLS-Older Males) | 5,020 | 1966 | 1990 | X | X | ||||
| National Nursing Home Survey Follow-up (NNHSF) | 6,001 | 1984 | 1990 | X | |||||
| National Social Life, Health, and Aging Project (NSHAP) | 3,004 | 2005 | Pres | X | X | X | X | ||
| The National Survey of Families and Households (NSFH) Reinterview | 13,017 | 2001 | 2003 | X | X | ||||
| National Survey of Self-Care and Aging: Baseline and Follow-up | 3,485 | 1990 | 1994 | X | |||||
| The National Survey of the Japanese Elderly (NSJE) | 3,990 | 1987 | 1993 | X | X | ||||
| STUDY FEATURES | ||||||||
| DATABASE | Baseline Sample Size | Start Year | End Year | Longitudinal | International | Minority Oversample(s) | Anthropometric Measures | Biospecimens |
| New Beneficiary Survey (NBS) and New Beneficiary Follow-up (NBF) | 16,692 | 1982 | 1991 | X | ||||
| New Immigrant Survey (NIS) | 13,981 | 2003 | 2004 | X | X | |||
| Nihon University Japanese Longitudinal Study of Aging (NUJLSOA) | 4,997 | 1999 | 2003 | X | X | |||
| Panel Study of Income Dynamics (PSID) | 65,000+ | 1968 | Pres | X | X | |||
| PHSE Ten-Year Follow-up of the North Carolina EPESE | 4,162 | 1996 | 1997 | X | X | |||
| Precursors of Premature Disease and Death | 1,337 | 1946 | 2003 | X | ||||
| Project TALENT | 440,000 | 1960 | X | X | X | |||
| 1990 Public Use Microdata Sample for the Older Population (PUMS-O) | Unknown | 1990 | 2000 | |||||
| Puerto Rican Elderly Health Conditions | 4,291 | 2002 | 2007 | X | X | X | X | |
| RAND Metadata Repository Religion, Aging, and Health Survey | 1,500 | 2001 | 2004 | X | X | |||
| Resources for Enhancing Alzheimer’s Caregiver Health (REACH) and REACH II | REACH: 600 REACH II: 642 | 1996 | 2004 | X | X | |||
| Sacramento Area Latino Study on Aging (SALSA) | 1,789 | 1996 | Pres | X | X | X | X | |
| Seattle Longitudinal Study (SLS) of Adult Cognitive Development | 6,000+ | 1956 | Pres | X | X | |||
| The Second Malaysian Family Life Survey (MFLS-2) | Senior sample: 1,357 | 1988 | 1989 | X | ||||
| Social Environment and Biomarkers of Aging Study (SEBAS) in Taiwan | 1,023 | 1999 | 2006 | X | X | X | X | |
| Study of Dementia in Swedish Twins | 3,838 | 1990 | 1999 | X | X | X | ||
| Study on Global Ageing and Adult Health (SAGE) | 90,000+ | 2002 | Pres | X | X | X | X | |
| Survey of Health, Ageing and Retirement in Europe (SHARE) | 31,115 | 2004 | Pres | X | X | X | ||
| Survey of Health, Ageing and Retirement in Israel (SHARE-Israel) | 2,598 | 2005 | Pres | X | X | X | ||
| Swedish Adoption/Twin Study of Aging (SATSA) | 2,020 | 1984 | 2005 | X | X | X | X | |
| Terman Life-Cycle Study, as supplemented | 1,528 | 1922 | 2000 | X | ||||
| The Wechsler Adult Intelligence Scale Archives (NIA-WAIS) on Aging and Multiple Cognitive Abilities | 50,000+ | 1980 | 1998 | X | ||||
| Whitehall II Study (also known as Stress and Health Study) | 10,308 | 1985 | Pres | X | X | X | X | |
| Wisconsin Longitudinal Study (WLS) (graduates) | 10,317 | 1957 | Pres | X | X | X | ||
| Wisconsin Longitudinal Study (WLS) (siblings) | 4,778 | 1975 | Pres | X | X | X | ||
| The Women’s Health and Aging Study (WHAS I, WHAS II, WHAS III) | 1,002; 436; 1,438 | 1992 | Pres | X | X | X | ||
| DATA SETS TO BE ARCHIVED IN THE FUTURE | ||||||||
| NIA Collaborative Studies on Dementia Special Care Units (SCUs) | 3,000 Nursing Homes 1,500 SCUs | 1991 | 1996 | X | ||||
| Origins of Variance in the Old-Old: Octogenarian Twins (The OCTO Twin Study) | 351 Same-SeX Twin Pairs | 1997 | 2005 | X | X | X | ||
| Victoria Longitudinal Study | 1,594 | 1987 | Pres | X | X | X | X | |
| DATA SETS AVAILABLE THROUGH PRINCIPAL INVESTIGATOR | ||||||||
| Epidemiology of Aging and Physical Functioning | 2,092 | 1993 | 2006 | X | X | |||
| The Longitudinal Study of Aging Danish Twins | 4,371 | 1995 | 2005 | X | X | X | X | |
| Maine-Syracuse Longitudinal Study | ~2,400 | 1975 | Pres | X | X | X | ||
| The UAB Study of Aging: Mobility Among Older African-Americans and Whites | 1,000 | 1999 | 2008 | X | X | X | ||
| The UNC Alumni Heart Study | 6,340 | 1986 | Pres | X | ||||
| Vietnam Era Twin Study of Aging (VETSA) | 1,006 | 2002 | Pres | X | X | X | ||
SOURCE: National Institute on Aging (2012).
working with partners in other countries to coordinate the collection of comparable cross-national data to understand the epidemiology of health and aging (see Box 9-1). The National Institute of Child Health and Human Development (also part of NIH) and the National Science Foundation fund the University of Minnesota to maintain the Integrated Public Use Microdata Series-International (IPUMS-International), an effort to inventory, preserve, harmonize, and disseminate census microdata from around the world
BOX 9-1
International Health Studies
of the Population Age 50 and Older
International surveys of the population age 50 and older serve as good models of harmonization and collaboration in the production of comparable health information across a number of countries. The United States began this effort with the Health and Retirement Study (HRS) in 1992. HRS, which is administered by the University of Michigan, surveys a representative sample of more than 26,000 Americans over the age of 50 every 2 years. It now has 11 waves of data. It is supported by the National Institute on Aging and the Social Security Administration. The English Longitudinal Study on Ageing (ELSA) began in 2002 with a sample of about 12,000 people age 50 and older and now has had five waves of data collection. The Survey of Health, Ageing and Retirement in Europe (SHARE) is a cross-national panel database with four waves of data for more than 55,000 individuals age 50 or older from 20 European countries. A number of additional countries throughout the world are now undertaking studies that will be part of this family of surveys.
These surveys have been developed collaboratively across countries and across disciplines: there is significant overlap in the memberships of their monitoring committees and advisory groups and active investigators. Producing comparable international data has been an aim since their beginning. The multidisciplinary approach allows comparable cross-national examination across a wide variety of health outcomes, as well as comparison of the strength of associations with causal or related variables. All of these studies have collected information on health conditions, disability, physical functioning, cognitive functioning, risk factors, and health care use and expenditures. They also collect extensive socioeconomic, demographic, and life-style factors, as well as information on earlier life events. All three surveys measure functional status, and HRS and ELSA collect biomarkers. SHARE is now piloting biomarker collection.
(University of Minnesota, 2012b).1 The project includes the Integrated Health Interview Series, which compiles a harmonized set of microdata and documentation based on material originally included in the public-use files of the National Health Interview Survey (University of Minnesota, 2012a).
Despite these impressive efforts, many of the data we sought for this report were scattered across disparate and sometimes obscure sources, and the data often did not exist, were inconsistently defined, or were contradictory. These limitations were often too great to allow us to reach definitive conclusions. We considered what steps the scientific community should take so that future analysts might benefit from a more robust body of evidence. Much of what can be done is beyond the scope of a single chapter to catalogue, but we offer three recommendations, beginning with one on the need for better data.
RECOMMENDATION 1: Acting on behalf of all relevant data-gathering agencies in the U.S. Department of Health and Human Services, the National Institutes of Health and the National Center for Health Statistics should join with an international partner (such as the OECD or the World Health Organization) to improve the quality and consistency of data sources available for cross-national comparisons. The partners should establish a data harmonization working group to standardize indicators and data collection methodologies. This harmonization work should explore opportunities for relevant U.S. federal agencies to add questions to ongoing longitudinal studies and population surveys that include various age groups—especially children and adolescents—and to replicate validated questionnaire items already in use by other high-income countries.
A fundamental challenge to understanding the U.S. health disadvantage is a lack of data to identify, monitor, and analyze epidemiological changes over time. Ambiguities in how best to define and measure health outcomes and determinants of health and inconsistent measurements across countries plague any effort to compare countries on meaningful terms. In some cases, the epidemiological literature has not even confirmed a causal link between
_________________
1The database currently includes approximately 397 million people, from 185 censuses taken in 62 countries from 1960 to the present.
some putative causes and associated health outcomes.2 Questions that have been validated in one country may perform differently in other countries, where life-styles, culture, or different meanings in translation can affect the results. Across topic areas, some countries participate in population surveys while others do not. These heterogeneities are an impediment to many efforts to make valid comparisons of health outcomes, determinants of health, and relevant contextual factors between one country and another. Thus, our first recommendation focuses on the need for better data, with an emphasis on the health outcomes discussed in this report, and on the determinants of health we reviewed, including health systems, personal behaviors, social and demographic factors, and physical and social environments.
Health Outcomes
Vital Statistics
Although vital statistics are available for nearly all of the populations of high-income countries and arguably measure the most precise endpoints imaginable—birth and death—attributions of cause of death still have inherent imprecision. For example, infant mortality comparisons are affected by differences in how countries register premature births and whether they are reported as live births. Cause-of-death attributions also may vary by country (e.g., “drug-related” deaths and suicides).
Physical Illnesses
Existing indicators do not go far enough to make meaningful cross-national comparisons of disease profiles of countries. For example, 30-day case-fatality rates assembled by the OECD focus on cross-national comparisons for only two conditions, acute myocardial infarction and stroke (OECD, 2011b). Similar data are needed for other major causes of death, and follow-up beyond 30 days is important to evaluate the quality of ambulatory and chronic illness care and readmission rates. Internationally comparable data are needed on the prevalence of ambulatory-sensitive conditions beyond the current focus on asthma and diabetes.
_________________
2Examples include precise quantification of the role of diet in causing cardiovascular disease, cancer, and other conditions; disentangling the effects of physical activity independent of obesity and diet; and which forms of “problem drinking” are predictive of disease or injury. Questions also surround the relative contribution of medical care to health outcomes and the causal role of stress, population-based services, and levels of public spending.
Mental Illnesses
As discussed in Chapter 2, deficiencies in available data and inconsistencies in diagnostic classifications prevented the panel from reaching conclusions about whether mental illness is more common in the United States than in other peer countries. Continued efforts are needed to standardize the collection of epidemiological data on mental illness based on established diagnostic instruments (see Chapter 2). An accepted international standard is lacking not only for established mental illnesses such as clinical depression, but also for relevant psychological factors, such as stress.
Determinants of Health
Health Systems
Cross-national comparisons of health system performance have been widely attempted (Davis et al., 2010), but they remain rudimentary. Validated indicators exist for delivery of specific services, such as those used for performance measures, but not for other dimensions of care important to outcomes, including measurements of the quality of care coordination for chronic illnesses or the quality of communication between providers and with patients. As discussed in Chapter 4, the only currently available systematic data to compare the quality of health care in countries come from surveys administered by the Commonwealth Fund, which are fielded in only 7-11 countries and rely on the perceptions of patients and primary care providers. Differences in cultural norms and expectations may skew patients’ responses to questions about whether doctors “spend enough time,” make mistakes, or communicate well. Developing more objective measures of quality, coordination, and communication that can be administered consistently across countries and can also account for contextual factors (e.g., differences in health systems and social policy) will require a collaborative effort among health services researchers from high-income countries.
For medical and public health systems among countries, no established (let alone validated) measures for access or quality are in use, apart from efforts to define the core content of public health, such as the core functions or the accreditation criteria recently developed in the United States by the Public Health Accreditation Board (Institute of Medicine, 2012) (see Chapter 4). Even national spending in these areas is difficult to compare: countries differ in both how they track spending on public health or social programs and how they classify these spending categories.3 Community-level
_________________
3For example, countries differ in what is classified as public health, prevention, health promotion, primary care, and social transfers.
financial data to assess population health investments are generally lacking. The Institute of Medicine (IOM) has made recommendations about the need to develop validated measures of public health services, including systems to track quality and accountability in public health departments (Institute of Medicine, 2011e, 2012). This work could inform the development of metrics to compare the core competencies of countries in providing public health services to their populations.
Personal Behaviors
Inconsistencies and ambiguous indicators also plague comparisons of how people behave in different countries. As noted in Chapter 5, a variety of questions have been asked about physical activity, diet, sexual practices, drinking, driving practices, and violence. Some questions have not undergone adequate scientific validation, rely on different sampling or survey administration protocols, or are interpreted differently across populations. For example, “leisure-time activity” and “total physical activity” are not constants across cultures.4 In addition, the degree to which such behavior predicts health outcomes among countries is unclear.
Similarly, international differences in dietary habits, menus, and even norms for portion sizes make it difficult to compare food consumption patterns. To our knowledge, comparable international data are lacking to compare injurious behaviors, such as driving while intoxicated; the failure to use seatbelts or child safety seats; or reckless acts that lead to poisoning, falls, drowning, fires, or burns. Few indicators exist for measuring the prevalence of injurious behaviors (e.g., fights), making it difficult to disentangle the role of weapons (e.g., firearms) in understanding high homicide rates in the United States. The leading drugs of abuse may vary across countries, and the focus of substance abuse surveys may therefore differ.
Social and Demographic Factors
Demographic and socioeconomic data (e.g., race and ethnicity, income) would have to be collected more systematically to make valid cross-national comparisons, such as comparing people of a given income level in one country with people of a similar income level in another country. Many U.S. surveys do not even ask about income or education, lack consistency in response options, or list broad income ranges that fail to meaningfully differentiate the purchasing power of different populations.
_________________
4Survey instruments like the International Physical Activity Questionnaire (Bauman et al., 2009) hold promise as a standardized tool for assessing physical activity.
Physical Environment
Chapter 7 discusses the limited availability of environmental data to compare physical and chemical exposures across countries or to document differences in land use and the built environment. Accepted metrics of the built environment that are applicable across different countries will be challenging to devise.
Social Environment
Even greater challenges to generalizability affect research efforts to compare countries in terms of social capital, social cohesiveness, and social participation. To begin such research will require agreement on accepted metrics, as well as the capacity to pose such questions in population studies.
Age Groups
Many of the data sources for the seminal studies on the U.S. health disadvantage—SHARE, ELSA, and HRS—were studies of aging that focused on adults age 50 and older. A pressing research priority is to define indicators and capture data for younger people and for each stage of the life cycle. Particular priority should be given to data on the health and behavior of children and adolescents (e.g., diet, exercise, alcohol and other drug use, driving, sexual activity) and related contextual variables. Such data are often lacking for children and adolescents (Institute of Medicine and National Research Council, 2011). Just as surveys such as SHARE provide morbidity data to measure the prevalence of diseases in adults over age 50, surveys are needed to make cross-national comparisons of morbidity, risk factors, and biomarkers in children, adolescents, and young adults.
The Maternal and Child Health Life Course Research Network (2012) is a recently established network of investigators who are committed to such an effort. Such development work is important to identify appropriate indicators to measure at each phase of the life cycle and to begin expanding understanding of the important influences that foster (or prevent) the development of risk behaviors, pathophysiological disease processes, and emotional turmoil. Children may be affected by a host of different environmental factors than are adults, and those effects may have different levels of significance in different life stages and settings.
Some of the important determinants of health are not conventional public health measures. For example, the Early Development Inventory and community “dashboards” created by Halfon and colleagues (e.g., Halfon et al., 2010) are data tools that help evaluate children in terms of social and emotional development, approaches to learning, language skills, and
cognition. Such indicators will need to be validated and used consistently across countries so that surveys can capture data on how differences in exposures may explain cross-national differences. Surveys will need to ask age-appropriate questions to create a temporal understanding of the major health determinants for each stage of the life course. As shown in Figure 9-1, a social-ecological interaction is occurring at age each stage of life, and the challenge of sophisticated longitudinal study of this process is to evaluate the effects of an evolving cast of potential influences at each stage.
Measures of adolescent health deserve particular attention because this is the life-cycle stage when so many nonmedical determinants of health come into play and when many life-long health behaviors are established. The infant mortality rate has long been regarded as an indicator of human development, as well as of the state of a nation’s public health (Lee et al.,
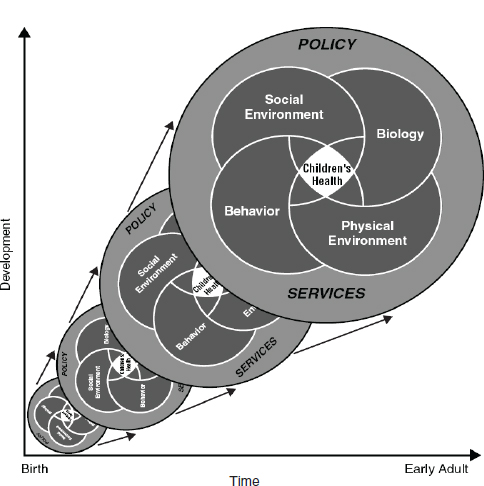
FIGURE 9-1 Social--ecologic influences on children’s health over time
SOURCE: National Research Council and Institute of Medicine (2004, Figure 2-2).
1997). Given that infant and early childhood mortality have fallen in all countries and that adolescent mortality exceeds child mortality in all high-income countries, adolescent mortality may be emerging as a stronger indicator of healthy human development for these countries (Viner, 2012).
Challenges and Opportunities
International Collaboration
Although harmonized data collection across multiple countries faces a variety of challenges, some inconsistencies are surmountable simply by agreeing to coordinate methods and to agree on harmonization proactively (“input harmonization”) rather than after the fact (Hoffmeyer-Zlotnik and Harkness, 2005). Relatively immediate steps (pursuing the “low-hanging fruit”) and long-term planning would be possible through a consortium of statistical officials from major countries who meet regularly and are committed to data harmonization. Interest in such efforts is increasing, and a number of harmonization efforts are already under way, including some with a particular focus on social determinants of health. A partial list of such global efforts is provided in Box 9-2. These efforts have received enthusiastic endorsement from world leaders, including a landmark September 2011 decision by the United Nations (2012a) General Assembly.5
A logical U.S. partner for international collaboration is the NIH, which has a deep interest in understanding the U.S. health disadvantage and in establishing a common data set that all countries could use for investigating and monitoring cross-national health differences. Such data are important to NIH not only to explain the U.S. health disadvantage, but also to expand knowledge of the biological and social determinants of disease over the life course. Other agencies in the U.S. Department of Health and Human Services share this interest—such as the Centers for Disease Control and Prevention (CDC)—and bring unique resources to the task of collecting and analyzing health data in the United States and overseas. The panel therefore
_________________
5The United Nations (2012a) General Assembly voted for the following action item in its resolution on noncommunicable diseases (e.g., heart disease, cancer): “Call upon WHO, with the full participation of Member States, informed by their national situations, through its existing structures, and in collaboration with United Nations agencies, funds and programmes, and other relevant regional and international organizations, as appropriate, building on continuing efforts to develop before the end of 2012, a comprehensive global monitoring framework, including a set of indicators, capable of application across regional and country settings, including through multisectoral approaches, to monitor trends and to assess progress made in the implementation of national strategies and plans on non-communicable diseases …,” see Rio Declaration in Box 9-2.
BOX 9-2
International Efforts to Harmonize Data
The European Commission (EC) has a commitment to “produce comparable data on health and health-related behaviour, diseases and health systems … to be based on common EU [European Union] health indicators, for which there is Europe-wide agreement regarding definitions, collection and use” (European Commission, 2012). Of 88 health indicators, the EC has identified more than 40 core indicators on demographic and socioeconomic conditions, health status, health determinants, and interventions (including health services and health promotion) for which data are “readily available and reasonably comparable” (European Commission, 2012). As part of the Public Health Program of its Directorate for Health and Consumers, the EC has made a long-standing commitment to data harmonization in Europe. The Public Health Program has a separate strand, with a separate budget, for improving health monitoring systems, from which many initiatives have received funding (European Commission, 2012). Examples of such activities include the European Health Survey System (which aims to harmonize health interview surveys) and the European Health Examination Survey (which prepares a harmonized health examination survey in 14 European countries).
The OECD is also active in promoting data harmonization, with a focus on the creation of comparable health care accounts and other indicators. This report, which cites OECD data extensively on a broad variety of issues, has been a beneficiary of the organization’s efforts to compile extensive cross-national data sets.
The European Observatory on Health Systems and Policies promotes evidence-based health policy making by studying health systems in more than 50 countries in Europe and elsewhere. This project represents a collaboration between the governments of nine European countries, the EC, the European Investment Bank, the World Bank, UNCAM (French National Union of Health Insurance Funds), the Regional Office for Europe of the World Health Organization (WHO), the London School of Economics and Political Science, and the London School of Hygiene and Tropical Medicine (European Observatory on Health Systems and Policies, 2012).
The Eurothine project, based at Erasmus University in Rotterdam (Erasmus, 2012), is “collecting and analyzing information from different European countries that will help policy-makers at the European and national level to develop rational strategies for tackling socioeconomic inequalities in health.” It is developing and collecting indicators of health inequalities to provide benchmarking data on inequalities to participating countries, along with assessing evidence and making recommendations on policy interventions. It intends to disseminate the results and to
“develop a proposal for a permanent European clearinghouse on tackling health inequalities.”
The World Alliance for Risk Factor Surveillance is working to finalize a definition and conceptual framework for behavioral risk factor surveillance that “can be shared and discussed globally” and “serve as a reference for researchers, practitioners, and countries that are developing behavioral risk factor surveillance” (International Union for Health Promotion and Education, 2009).
The Washington Group on Disability Statistics was formed as a result of the UN International Seminar on Measurement of Disability, which occurred in New York in 2001. An outcome of that meeting was the recognition that statistical and methodological work was needed at an international level to facilitate the comparison of disability data cross-nationally. Consequently, the UN Statistical Commission authorized the formation of a “city group” to address some of these issues and invited the National Center for Health Statistics in the United States to host the group’s first meeting. The city group format typically involves three or four working meetings at which representatives from national statistical agencies address selected problems in statistical methods. The Washington Group on Disability Statistics takes its name from the location of the group’s first meeting (Centers for Disease Control and Prevention, 2009e).
In 2011, WHO issued the Rio Declaration on Social Determinants of Health, which included a commitment to 12 strategies of data collection, listed below. The declaration (World Health Organization (2011c, p. 6) noted:
that monitoring of trends in health inequities and of impacts of actions to tackle them is critical to achieving meaningful progress, that information systems should facilitate the establishment of relationships between health outcomes and social stratification variables and that accountability mechanisms to guide policy-making in all sectors are essential, taking into account different national contexts.
The Rio Declaration was adopted by WHO Member States in 2012 at the Sixty-fifth World Health Assembly in Geneva, Switzerland. It includes 12 pledges to monitor progress and increase accountability (World Health Organization (2011c, pp. 6-7):
1. Establish, strengthen and maintain monitoring systems that provide disaggregated data to assess inequities in health outcomes as well as in allocations and use of resources;
2. Develop and implement robust, evidence-based, reliable measures of societal well-being, building where possible on existing indicators, standards and programmes and across the social gradient, that go beyond economic growth;
3. To promote research on the relationships between social determinants and health equity outcomes with a particular focus on evaluation of effectiveness of interventions;
4. Systematically share relevant evidence and trends among different sectors to inform policy and action;
5. Improve access to the results of monitoring and research for all sectors in society;
6. Assess the impacts of policies on health and other societal goals, and take these into account in policy making;
7. Use intersectoral mechanisms such as a Health in All Policies approach for addressing inequities and social determinants of health; enhance access to justice and ensure accountability, which can be followed up;
believes that the role of coordinating these efforts should logically occur at the departmental level and not any one agency.
Data Access
Another opportunity for overcoming the limitations of data is to broaden access to existing data sets. The open government movement in the United States shares this aim. A secure publicly accessible data warehouse platform to enable investigators to access data for cross-national comparisons is a research priority well within the capabilities of modern information systems architecture. The widely used Luxembourg Income Study (LIS) has been identified as a particularly strong model worthy of replication in the health field (Bambra and Beckfield, 2012, pp. 31-32):
Several key characteristics of the LIS make it a perfect model for a comparative database on population health: researchers can access individual-level
8. Support the leading role of the World Health Organization in its collaboration with other United Nations agencies in strengthening the monitoring of progress in the field of social determinants of health and in providing guidance and support to Member States in implementing a Health in All Policies approach to tackling inequities in health;
9. Support the World Health Organization on the follow-up to the recommendations of the Commission on Information and Accountability for Women’s and Children’s Health;
10. Promote appropriate monitoring systems that take into consideration the role of all relevant stakeholders including civil society, nongovernmental organizations as well as the private sector, with appropriate safeguard against conflict of interests, in the monitoring and evaluation process;
11. Promote health equity in and among countries, monitoring progress at the international level and increasing collective accountability in the field of social determinants of health, particularly through the exchange of good practices in this field; and
12. Improve universal access to and use of inclusive information technologies and innovation in key social determinants of health.
data (critical for examining social inequality), access is via remote server (LIS requires application for permission to access the data, but a researcher never “owns” the data, which allows for the free dissemination of sensitive information), and the LIS team harmonizes the data to aid in international comparison (just as the LIS developed an “income concept” to facilitate comparison, likewise a “health concept” could be developed for comparative analysis)…. [W]e think the development of such a rich resource for the scientific community is the top priority for new science on these critical questions. The sort of detailed comparative research on health that Elo (2009) and others have called for simply cannot be conducted in a way that allows knowledge to cumulate without such data infrastructure.
Expanding Current Surveys
Another important opportunity to enhance data is to add new questions (or replace outdated questions) on existing longitudinal or cohort studies and on national population surveys, such as the National Health
and Nutrition Examination Survey and BRFSS,6 with a focus on variables relevant to health determinants and life-cycle influences at all ages that may help to explain the U.S. health disadvantage. Such efforts would serve two important purposes. First, expanding the data collected would provide an opportunity for U.S. surveys to include questions already in use in Europe and elsewhere, thereby enabling prevalence rates in the United States to be accurately compared with those of other countries. For example, only minor modifications are needed to align questions about sexual behavior on the Youth Risk Behavioral Survey (YRBS) and the Health Behaviour in School-Aged Children (HBSC) survey. Similar modifications could occur with other surveys, such as harmonizing the National Longitudinal Survey of Youth (NLSY) with questions asked in other countries. Second, an expansion would provide data that investigators could use to study the causal pathways responsible for health in general and the U.S. health disadvantage in particular.
Cross-National Surveillance
In addition to expanding the collection of survey data in the United States, the National Center for Health Statistics and the CDC could maintain an ongoing effort to look abroad to track how efforts to improve public health in the United States compare with those in other countries. Regular reports—such as those that appear in the Morbidity and Mortality Weekly Reports (MMWR) and are reprinted in the Journal of the American Medical Association and by many news outlets—would be an appropriate vehicle for publishing updates on U.S. health rankings and health statistics relative to other high-income countries. This ongoing surveillance would help to monitor progress and identify opportunities to learn from successes in other high-income countries. For example, the Transportation Research Board (TRB) gleaned important insights from other countries on strategies that could be used to reduce traffic fatalities in the United States (see Chapter 8). This is not to say that other countries have all the answers; but their experiences suggest strategies and approaches that might also work in (parts of) the United States or that can be adapted and piloted in the United States.
It will be important to continue to compare health rankings for population subgroups (e.g., by socioeconomic status, race and ethnicity, access to health care) to help differentiate the contribution (or lack thereof) of
_________________
6Supplementary modules administered by BRFSS provide a system that can adapt to needs and could be used to explore causal hypotheses about cross-national health differences. For example, questions added to these modules could collect data on such factors as injurious behaviors and the social and physical environment.
different factors in accounting for cross-national differences. Comparisons with England have already demonstrated that the U.S. health disadvantage appears to persist across racial and ethnic groups in the United States and among college-educated and upper income populations (Banks et al., 2006; Martinson et al., 2011a, 2011b), but the studies to date have their limitations. For example, the study by Banks et al. (2006) was restricted to adults aged 55-64. The stratified data described by Martinson and colleagues, which did not appear in their original article (2011a), could be analyzed more carefully in future studies that apply multifactorial regression analyses. Such analyses could be informed by new studies and better data, as they become available, to assign coefficients that more precisely quantify the relative contribution of different variables to the U.S. health disadvantage.
Logistical Challenges
Logistical and resource constraints may make it difficult to take these steps or to sustain data collection activities across countries or even within countries. Most data agencies are plagued by tenuous funding streams, and they often face other organizational and technological barriers to data collection. For example, the United States lacks the capacity to evaluate the public health services it provides to populations because those services are fragmented across federal health agencies, state health departments, and more than 3,000 local health departments. Because BRFSS is administered by states, which can elect which modules to administer, it is also an example of how decentralization (see Chapter 8) can limit the ability of the U.S. government to gather consistent national health statistics. A previous Institute of Medicine (2011e) study made extensive recommendations, directed to the National Center for Health Statistics and CDC, to undertake bold reforms in the scope and quality of public health data collected by the agencies. The recommendations included the need for a greater focus on social determinants of health, on community conditions that affect health, and on linking data systems in the public and private sector to create more informative “dashboard” data on health conditions at the national, state, and local level.
Methodological Challenges
Research efforts that rely on surveys must contend with different methods for sampling and administration and low, or at least inconsistent, response rates. For example, ELSA had a lower response rate than HRS, which can introduce a response bias. Some countries participating in SHARE had response rates below 50 percent at baseline. Nonrespondents may be more likely to be disadvantaged (and less healthy).
Much of the data compiled in this report relies on self-reported information
in population surveys (e.g., of diet, drinking habits, physical activity, medical errors). Methodological research should explore the use of biomarkers and objective reference standards to establish the validity of self-reported observations, such as the use of pedometers and global positioning system (GPS) data to validate self-reports of physical activity and the use of administrative and medical record data to validate reports of medical errors.
Cross-national comparisons treat countries as units of analysis, but from a policy and statistical perspective they are not truly independent because of cross-national ties, such as drug policies enforced by the European Union. The important distinctions may be less about geographic national borders than the relevant regions or populations within countries (Hans, 2009). For example, some argue that U.S. states are more appropriate units of comparison for cross-national studies because of the large size of the United States and significant state-level disparities in health status and other health-related variables.7
A further nuance for researchers to tease apart in cross-national comparisons is whether a risk factor, such as poverty or inadequate education, may have different “toxicity” (health implications) depending on the contextual circumstances in each country. For example, as discussed in Chapter 6, there is some evidence that the absence of a college education may have greater effects on employment and health in the United States than in other countries.
RECOMMENDATION 2: The National Institutes of Health and other research funding agencies should support the development of more refined analytic methods and study designs for cross-national health research. These methods should include innovative study designs, creative uses of existing data, and novel analytical approaches to better elucidate the complex causal pathways that might explain cross-national differences in health.
A daunting methodological challenge is how to design studies to understand the causes of the U.S. health disadvantage. Randomized controlled trials, which are considered the strongest evidence of effectiveness
_________________
7Similarly, like the United States, comparison countries also experience important health disparities by province or canton. It could be argued that an “apples to apples” comparison with the United States would contrast similar regions or, perhaps more meaningfully, would compare similar populations in each country, along with appropriate adjustments for relevant covariates affecting health.
in much medical research, are hardly the answer for this field (Anderson and McQueen, 2009; Black, 1996; Braveman et al., 2011c; Glasgow et al., 2006; McQueen, 2009; Petticrew and Roberts, 2003; Victora et al., 2004). Innovations in study designs require thoughtful methodological research and support from funding agencies to sponsor such efforts. The National Institutes of Health, other grant-making institutions, and public-private partnerships could play important roles in funding pilot studies and innovative methodological research to develop such designs in collaboration with colleagues in other countries.
Recent advances in analytic techniques enable researchers to answer more complex questions about the explanation of between-country differences in levels and trends of health indicators. These advances include techniques that allow improved causal inferences regarding population differences, such as multilevel analysis methods that account for factors at different levels of organization (e.g., countries, regions, and individuals) (see Diez Roux, 2011); instrumental variable and other approaches that improve causal inferences regarding population-level differences (see Ahern et al., 2009; Hernán and Robins, 2006); and systems modeling tools that allow one to integrate information from different sources and consider dynamic relations. Counterfactual analysis techniques (such as techniques based on population attributable fractions, which allow an assessment of the contribution of specific risk factors to variations in health outcomes between populations [Northridge, 1995]), fixed effects models, complex systems theory (Diez Roux, 2011), and econometric techniques are among the important tools available. In lieu of longitudinal studies, data fusion through statistical matching has been explored as a way of combining data for life-course research (D’Orazio et al., 2006; Rässler, 2002).
Longitudinal Research
Much of the evidence presented in this report consists of cross-sectional comparisons of mortality and prevalence rates in recent years, along with some historical trend data that span several decades for some indicators. The more important question in understanding the U.S. health disadvantage is to explore the relationship between antecedent factors and health outcomes, some of which occur relatively soon after a risk exposure (e.g., unintended pregnancies) and some of which transpire over years or decades. The life-course perspective embraced by this panel places a premium on understanding how the health problems experienced by Americans are shaped by their early life circumstances—and perhaps even the circumstances of their parents before they were born—and this approach obviously necessitates either prospective longitudinal studies or creative uses of historical data to retrospectively examine causal factors. Clues to the health
disadvantages experienced by today’s senior citizens may lie in (archived) post–World War II data on living conditions generations ago. Data to track all age groups are important, but longitudinal data that includes middle-aged adults appear to be especially lacking.
The United States is responsible for important longitudinal research, both historically (e.g., the Framingham Heart Study) and in ongoing studies. One example is the National Children’s Study (Hirschfeld et al., 2010), an effort to study the long-term experience of 100,000 children and their families that exemplifies such a commitment but has faced its own challenges. Other examples include the Panel Study of Income Dynamics, the longest running longitudinal household survey in the world (Institute for Social Research, 2011), and the National Longitudinal Surveys (U.S. Bureau of Labor Statistics, 2012).
However, the United States generally lags behind the investments other countries have made in conducting longitudinal research. Sweden has maintained an impressive longitudinal data set for more than a century. The Whitehall Studies in the United Kingdom, which began in the late 1960s, produced seminal data on the role of social determinants of health (Marmot et al., 1991). In New Zealand, the Dunedin Multidisciplinary Health and Development Study has been following 1,037 individuals for four decades, since their birth in 1972-1973. Other classic British cohort studies include the National Study of Health and Development (launched in 1946), the National Child Development Study (launched in 1958), and the British Cohort Study (launched in 1970).
Worldwide interest in identifying and measuring early life precursors of both health and socioeconomic outcomes has spawned the launch of “Millennium Cohort Studies” in many countries. These studies include the Danish National British Cohort (100,418 pregnant women, launched in 1996), the Norwegian Mother and Child Cohort (108,000 pregnant women, launched in 1999), the Dutch Generation R Study (9,748 pregnant women, launched in 2001), Born in Bradford, UK (14,000 pregnant women, launched in 2007), Growing Up in Australia (10,000 children, launched in 2004), Millennium Cohort Study U.K. (20,000 children, launched in 2001), the Étude Longitudinale Français Depuis L’Enfance (20,000 children across France, launched in 2011), and Growing Up in Scotland (8,000 children, launched in 2003, with a second wave of 8,000 children enrolled in 2008).8
The United States has opportunities to expand this genre of research by collecting prospective data on the influence of social factors on health
_________________
8The U.S. Department of Defense also launched a Millennium Cohort Study in 2001, which now involves approximately 150,000 participants, but its focus is on the long-term effects of military deployment.
outcomes. For example, for many years the research community has advocated the collection of longitudinal data by NHANES. Another option is to expand the Early Childhood Longitudinal Study (ECLS) by collecting data on health outcomes. The ECLS-K of 1998-1999 followed a nationally representative sample of more than 21,000 children who were kindergartners in 1998-1999 through the eighth grade. The ECLS-K program provides national data on children’s transition to school and their experiences and growth through the eighth grade. The ECLS program also provides data to analyze the relationships among a wide range of family, school, community, and child characteristics with children’s development, learning, and performance in school (National Center for Education Statistics, 2012a).
Mining Currently Available Data
Although a new wave of long-term longitudinal research is certainly needed, more can be done with the available data already in existence. At a time of limited resources for new research, funding agencies can achieve important economies by funding investigator-initiated studies that propose secondary analysis of existing data sets. For example, BRFSS data could be more effectively mined to uncover more valuable information than currently occurs. Important insights could be obtained by examining historical data because the U.S. health disadvantage has been growing over time and the important antecedents occurred decades ago. An important avenue the panel identified, which it did not have time to explore, would be to map historical trends in social factors, such as poverty and social capital, from post–World War II and to track their evolution over time as the U.S. health disadvantage has grown more pronounced.
In some cases, useful data for international comparisons may exist in disparate databases that are familiar only to specialists in certain disciplines. This report demonstrates the broad spectrum of disciplines relevant to understanding the U.S. health disadvantage, spanning health, social science, economics, and the environment. Even in the digital information era, an exhaustive search of all databases that provide a basis for making international comparisons is challenging. For example, this panel was not confident that it had adequately identified all possible data sources for comparing the physical and social environments in high-income countries. It is possible, for example, that specialists in air quality, climate, social networks, or other disciplines are aware of differences between the United States and other countries that we did not discover in our review.
Other opportunities exist in exploiting linked data sets, such as the National Death Index, which combines death records and survey data (Centers for Disease Control and Prevention, 2009c), and in conducting
secondary data analysis across multiple studies. For example, the Emerging Risk Factors Collaboration has established a central database on more than 2 million people from more than 125 prospective population-based studies (Emerging Risk Factors Collaboration, 2012). That collaboration’s focus is on risk factors for cardiovascular disease, but a similar model could be pursued to stratify the data by country in order to study determinants of a broader array of cross-national health differences.
Another opportunity exists in reinvigorating successful surveys that have not been fielded for many years and could be updated. For example, the most recent European data from HBSC survey are from 2005-2006 (Roberts et al., 2009). Data from that survey on children’s activity levels may not reflect current behaviors in an era in which use of electronic devices, video games, and smart phones has probably supplanted many outdoor play activities. In the United States, the National Maternal and Infant Health Survey (NMIHS) has not been conducted since 1988. Other similarly dormant surveys could be revived in a new effort to understand cross-national differences.
Discordant family designs are another intriguing model, because they enable statistical comparisons to be made within pairs of twins or clusters of siblings and can help quantify the role of environmental factors in health disparities. This design implicitly controls for confounding from factors that are constant within families and helps to disentangle the different contributions from adult socioeconomic position, childhood socioeconomic position, and genetic factors. Such studies have their limitations, including requirements for large sample sizes, the persistent inability to prove causation or eliminate confounding (e.g., from “ability bias”), random measurement error, and international generalizability (Madsen et al., 2010; McGue et al., 2010). However, these study designs remain useful to consider for appropriate research questions.
Funding agencies can support efforts by researchers to devise creative strategies to design and conduct such studies and to explore alternative study design concepts that can yield more immediate results. Such efforts have led to important findings. For example, important information about the role of smoking in explaining the U.S. health disadvantage among adults aged 50 and older (see Chapter 6) was derived from sophisticated modeling studies that relied on evidence based on smoking-attributable fractions (Preston et al., 2010a, 2010b). Further research could explore the validity of this method of estimating contribution to mortality for a variety of conditions and age groups.
RECOMMENDATION 3: The National Institutes of Health and other research funding agencies should commit to a coordinated portfolio of investigator-initiated and invited research devoted to understanding the factors responsible for the U.S. health disadvantage and potential solutions, including lessons that can be learned from other countries.
For reasons noted throughout this report, a meaningful effort to understand the U.S. health disadvantage requires multiple lines of inquiry and a long time horizon, which in turn will require ongoing financial and political support. Long-term cohort studies, and even elaborate retrospective studies, require an investment of time and committed funding to sustain data collection over many years. Although financial constraints make long-term commitments to research very difficult, the persistence (and worsening) of the U.S. health disadvantage over decades, with its profound human and economic implications, may justify such an investment. The knowledge gleaned from such research has the potential not only to help the United States regain its footing as a leader in health and improve its long-term economic outlook but also to broaden universal understanding of the factors responsible for cross-national health differences.
The cause-effect relationships for some aspects of the social and other nonmedical determinants of health are not yet well established. Knowing and understanding causal pathways is a first step in devising appropriate policies, but the question of attribution remains. As Deaton (2002, p. 15) argues: “policy cannot be intelligently conducted without an understanding of mechanisms; correlations are not enough.”9 A particular suite of questions is especially important in understanding why the United States is experiencing a health disadvantage relative to other countries. We resist the temptation to prioritize the research questions—such as arguing that the study of social determinants is more important than comparing the role of health care systems—because we recognize the fallacy of predicting which lines of scientific inquiry will yield the greatest insights and propel the most important improvements in public health. To fill the gaps in scholarship on the subject, the panel envisions a portfolio of research supported by the National Institutes of Health and other funding entities, including the following:
• international tracking studies that maintain a current epidemiologic dashboard on cross-national patterns in the prevalence of diseases,
_________________
9In circumstances in which a clear cause-effect relationship cannot be linked with a discrete policy intervention, there may still be a valid policy argument for pursuing interventions based on other values, with causal mechanisms only partially understood.
biomarkers, and risk factors; all-cause and cause-specific mortality rates; and the incidence of injuries for key age groups (especially for people under age 50), by administering the same instrument in a standard group of high-income countries;
• further research on how the U.S. health disadvantage is distributed by income and education and what factors may be responsible for the differential influence of income on health;
• long-term prospective cohort studies and other innovative designs (e.g., twin and family studies) that could document the role of antecedent factors (policy, the environment, social factors, behaviors, and health systems) on the U.S. health disadvantage;
• questions about past experiences and exposures (retrospective questions)10 on population surveys, which can facilitate research on life-course influences (although validation of such questions may require longitudinal studies);
• retrospective studies of historical data and time-series analyses to better elucidate how past conditions in the United States might help explain current health patterns;
• environmental measurement to understand place-based influences on cross-national health disparities, including the effect of land use and urban planning decisions in cities and contextual factors in the large rural areas of the United States;11 and
• area-based research using geocodable data, geographic information systems (GIS) technology, and a variety of newer approaches based on global positioning.
This report has identified a series of important research questions that deserve exploration, too many to list here. However, it is important to note some of the crucial unanswered research questions about the U.S. health disadvantage:
• What specific factors explain the unfavorable birth outcomes (e.g., high infant mortality rates) experienced in the United States, which exist even after adjusting for race, ethnicity, and maternal education?
_________________
10Examples include the National Survey of Family Growth and National Longitudinal Study of Youth.
11Important areas for future research include characterizing levels and distributions of environmental risk factors using comparable measures across countries, documenting inequalities in the distribution of these environmental factors, and identifying the extent to which these environmental factors affect health and the extent to which their effects are modulated by individual-, community-, or country-level factors.
• To what extent does inadequate health care explain why Americans are more likely than their counterparts in peer countries to die from:
o transportation-related injuries
o violence
o noncommunicable diseases
o communicable diseases
• What specific factors explain why the United States has a higher obesity rate than any other high-income country?
• Do firearms alone explain the excessively high homicide rate in the United States, including murders of children?
• What accounts for the “drug-related” deaths that claim a large proportion of excess years of life lost in the United States?
• What specific factors explain why U.S. adolescents have a higher rate of pregnancies and abortions than their counterparts in other high-income countries?
• Why does the United States have the highest rate of AIDS among OECD countries?
• Is mental illness generally, and are specific mental illnesses, more common in the United States than in other peer countries?
• Why are Americans more likely than people elsewhere to describe their health as good or excellent?
• Why do Americans have a health advantage for certain conditions (e.g., stroke), and can the answers to that phenomenon help explain the causes of health disadvantages for other conditions?
• To what extent do social and economic inequality and low social mobility, independent of absolute poverty, contribute to the aggregate disadvantage in U.S. health?
• To what extent do working conditions in the United States differ from those in peer countries, and how might these contribute to the U.S. health disadvantage?
• Are advantaged Americans—by race (e.g., non-Hispanic whites), education, income, insurance status, and risk factors (e.g., nonsmokers, nonobese)—in worse health than their counterparts in other countries as some research suggests?12 If true, does the finding
_________________
12Four studies have now reported this pattern (Avendano et al., 2009, 2010; Banks et al., 2006; Martinson et al., 2011a), but some of them looked only at education and not other variables (Avendano et al., 2010), or are restricted to comparisons of a narrow age group in only two countries (Banks et al., 2006). Replication with more focused criteria would help confirm the finding.
apply to only some of the health conditions for which the United States is experiencing a disadvantage?13
• To what extent do epigenetic processes help explain the links between environmental factors and the biological outcomes observed in the U.S. health disadvantage?
• To what extent does the United States lack “protective factors” that buffer the effects of adverse factors, from poverty to adolescent pregnancy?
Stable Funding
Conditions that encourage investigators to commit themselves to long-term lines of inquiry require confidence in a stable source of funding for competitive applications. Solicitations for proposals that are expected to achieve specific aims within 3-5 years discourage ambitious enterprises, like the National Children’s Study, which follow individuals over their life courses. Another limitation is lack of “ownership” of the problem: no entity in government is responsible for studying the U.S. health disadvantage.
Creating an institutional home for such research in the Office of the Director of NIH would give the effort a strategic position to coordinate the research portfolios across the agency’s 27 institutes and centers, to support inclusion of measures from OECD and European studies in relevant NIH-funded studies, and to solicit proposals for developing measures, data collection instruments, and sampling and administration methodologies. Other potential institutional homes include the Office of Global Health at CDC and the U.S. Department of State. Academic centers of excellence, such as the CDC prevention centers, or academic institutions with expertise on social determinants of health, could be further expanded with appropriate funding to study the underlying causes of the U.S. health disadvantage.
Perhaps the largest impediments to furthering research on comparisons of cross-national health are the data collection capacities of countries. Not all countries are positioned, or can afford, to administer large-scale population surveys on an annual basis and to maintain publicly available data repositories for research use by the scientific community. Impediments include limited budgets, pragmatic and bureaucratic constraints, and the absence of international collaborative arrangements. In the United
_________________
13Further research is needed to know whether the higher rates of disease for certain conditions in the United States, such as HIV infection, are differentially distributed across social classes.
States, for example, funding for the National Children’s Study has met with numerous challenges (Wadman, 2012). Countries can sometimes field large surveys, but not on a regular basis. Political considerations can also influence research by dictating what gets measured and who decides.
Another challenge is the shortage of qualified investigators to conduct such research. Tenuous funding opportunities affect the training pipeline and discourage young investigators from pursuing research careers directed at the issues covered in this report. Dedicated funding for a research portfolio that includes career development awards and support for investigator-initiated studies would help to change this climate, not to mention the motivation to undertake protracted longitudinal studies.
Calls for research in this field by NIH, in particular, would be very persuasive in shifting attitudes in academia, and universities’ promotion and tenure committees might adopt more enlightened policies on scholarship that draw more young faculty into careers focused on these issues. Establishing special emphasis panels and study sections composed of reviewers with appropriate expertise and knowledge of the special methodological challenges in conducting cross-national comparative research (and who consider a wider range of analytic approaches, appropriate to the subject, than randomized controlled trials) would also cultivate career growth in this field. These changes in research culture might then find their way to professional journals and persuade editors to involve reviewers with appropriate expertise to make judgments about the worthiness of manuscripts for publication.
For their part, scientists and researchers who conduct studies of the U.S. health disadvantage—a topic with profound public policy implications—need to enhance their skills in communicating scientific findings to general audiences, to policy makers, and to stakeholders. These audiences do not generally read peer-reviewed journals or attend scientific meetings, and findings need to be presented in understandable formats and venues that are relevant to their decisions. Work by Marmot (e.g., 2010), Cutler (e.g., Meara et al., 2008), McGinnis (e.g., McGinnis et al., 2002), Woolf (e.g., Woolf, 2011), Lantz (e.g., Lantz et al., 2010), Schoeni (e.g., Schoeni et al., 2011), and Kindig (e.g., Kindig et al., 2010) among others, illustrates how to present scientific evidence about population health interventions—including returns on investment—to nonscientific policy audiences and decision makers who shape public policies.
The diversity of disciplines needed for studying and understanding the U.S. health disadvantage, ranging from biomedicine to political science, should compel scientists to enthusiastically embrace interdisciplinary collaborations. Medicine, public health, epidemiology, sociology, demography, behavioral science, economics, marketing, and other diverse disciplines and fields can all contribute to the study of the U.S. health disadvantage,
but they will need to work through differences in nomenclature, research traditions, data repositories, top journals, and key scientific meetings. Yet the collaboration of experts with different perspectives and skills produces insights that are greater than the sum of the parts and holds the greatest promise in solving the mysteries of the U.S. health disadvantage.
































