
Environmental Gases and Contact Lens Wear
Gerald E. Lowther
OXYGEN
Oxygen has been the most studied gas with respect to contact lens wear because the avascular cornea must obtain oxygen from the atmosphere. Without oxygen from the air, corneal swelling will occur, with resultant corneal clouding, decreased visual acuity, discomfort, and other long-term adverse effects. The cornea requires about 5 µl O2/mm2 cornea/hour (Hill and Fatt, 1963; Larke et al., 1981). This value varies with individuals from about 3 to 10 µl O2/mm2 cornea/hour (Larke et al., 1981).
Under open-eye conditions at sea level the anterior surface of the cornea has available about 20.9 percent oxygen (O2 in air) or about 155 mmHg partial pressure. With the eye closed the oxygen level drops to about 7 percent. With contact lens wear the lens will impede oxygen from reaching the cornea. Therefore, considerable effort has gone into developing lenses that will supply oxygen to the cornea. Oxygen can be supplied under a lens by designing the lens such that tear exchange occurs with each blink, bringing in oxygen dissolved in the tears. This usually does not supply enough oxygen. An exchange of about 10-15 percent of the tear volume under a rigid lens can occur with each blink (Figure 1) (Fatt and Hill, 1970; Fatt, 1969; Cuklanz and Hill, 1969), but with a soft (hydrogel) lens less than 2 percent exchange occurs (Polse, 1979; Wagner et al., 1980). Therefore, to supply adequate oxygen to the cornea, lens materials must allow oxygen diffusion.
The oxygen supplied through a contact lens can be measured and specified in different ways. One method is a physical one in which the lens material is placed in a chamber with one side exposed to air and a sensor is placed on the opposite side to measure the oxygen flow. With this method the Dk
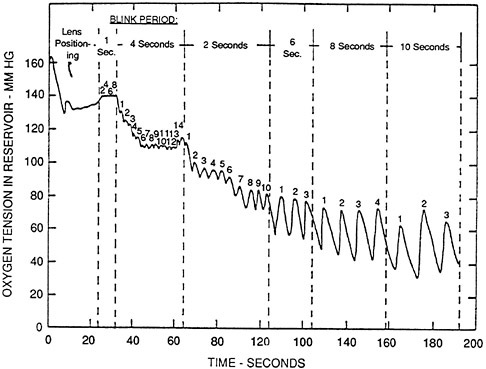
FIGURE 1 Oxygen tension under a rigid PMMA lens with different blink rates. SOURCE: Fatt and Hill (1970). Reprinted by permission.
value, termed permeability, is determined. The higher the Dk value the more oxygen will diffuse through a unit thickness of material. To determine the amount of oxygen that will diffuse through a given contact lens, the Dk value is divided by the lens thickness (L) to give a Dk/L value, which is called transmissibility. Clinically the transmissibility is the important value. The higher the value, the more oxygen will reach the cornea. Permeability is given as a number × 10−11 (cm22/sec)(ml O2/ml mmHg). Transmissibility is given as a number × 10−9 (cm/sec)(ml O2/ml mmHg). In both cases only the initial number is quoted with the units and power of 10 assumed.
Another method of specifying the amount of oxygen going through a lens is by the equivalent oxygen percentage or equivalent oxygen performance (EOP). This is a biological test in which a sensor is placed against the corneal surface and the rate of oxygen utilized from a membrane over the sensor is determined. The rate can be determined with the eye under different oxygen atmospheres. A contact lens can be placed on the eye for a period of time and then removed, and the oxygen uptake rate can be measured again. Using this method one can say that the cornea had an oxygen thirst equivalent of a given percentage of oxygen. The EOP values will be between
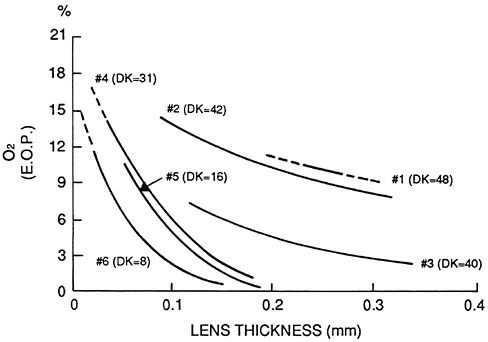
FIGURE 2 The relative equivalent oxygen percentage (EOP) of six hydrophilic contact lens materials over various ranges of lens thickness. A sample Dk value (see text) appears in parentheses for each in units multipled by 10−11 (cm2/sec) ml O2/ml × mmHg). SOURCE: Adapted from Hill and Mauger (1980).
0 percent and 20.9 percent. The higher the value the more oxygen transmitted through lens to the cornea. Plots are usually given as percent oxygen against lens thickness (Figure 2) (Hill and Mauger, 1980).
An important question is the minimum oxygen that the cornea requires. Another important factor is how much of the required oxygen does the available contact lens materials provide. In terms of oxygen percentage to prevent corneal changes, values from 1.5 percent up to 18 percent have been quoted (see Table 1). Holden et al. (1984) found an average of 10.1 percent to prevent any edema (Figure 3). Holden and Mertz (1984) found that with daily wear 9.9 percent oxygen was required, whereas with extended wear, to limit the edema to no more than the physiological 4 percent swelling, an oxygen percentage of 17.1 was required. When extended-wear lenses are worn, with resultant overnight swelling, one would like the swelling to decrease during the day to baseline levels. To accomplish this Holden and Mertz (1984) found that an EOP of 12.1 percent was required. The transmissibility values required are as follows (values calculated based on water content and thickness:
EOP 9.9% Dk/L 24.1
EOP 12.1% Dk/L 34.3
EOP 17.1% Dk/L 87.0
With present hydrogel lenses the Dk value is related to the water content (Figure 4) (Sarver et al., 1981). The highest Dk value possible is about 50. Transmissibility is therefore related to only the water content and lens thickness. Thus, with the present hydrogel materials the amount of oxygen that can be supplied is limited. Table 2 gives the Dk/L values for different water contents and lens thicknesses.
TABLE 1 Estimates of the Critical Oxygen Requirements (COR) of the Cornea
|
Author |
Year |
Criterion |
COR (%) |
|
Epithelium: Biochemical |
|||
|
Uniack et al. |
1972 |
Glycogen depletion |
5 |
|
Uniack et al. |
1972 |
LDH concentration |
5 |
|
Hill et al. |
1974 |
SDH reactivity |
5 |
|
Hamano et al. |
1983 |
Lactate |
<13.2 |
|
Epithelium: Structure/Function |
|||
|
Fatt |
1968 |
Oxygen consumption |
2.7 |
|
Uniacke et al. |
1972 |
Epithelial thickness |
5 |
|
Millodot and O'Leary |
1980 |
Sensitivity |
>7.7 |
|
Hamano et al. |
1983 |
Mitosis |
<13.2 |
|
Masters |
1984 |
Mitochondria |
>10 |
|
Benjamin and Hill |
1985 |
Oxygen consumption |
15.6 |
|
Stroma |
|||
|
Polse and Mandell |
1970 |
Corneal edema |
1.5–2.5 |
|
Carney |
1974 |
Corneal edema |
2 |
|
Mandell and Farrell |
1980 |
Corneal edema |
3.1 |
|
Mizutani et al. |
1983 |
Corneal edema |
15 |
|
Holden et al. |
1984 |
Corneal edema |
10.1 |
|
Mandell |
1985 |
Corneal edema |
7.4 |
|
Brennan et al. |
1987 |
Corneal edema (gas) |
10.9 |
|
Brennan et al. |
1987 |
Corneal edema (EOP) |
18.0 |
|
Endothelium |
|||
|
Williams |
1986 |
Bleb response |
16.6 |
|
Source: Effron and Brennan (1987). |
|||
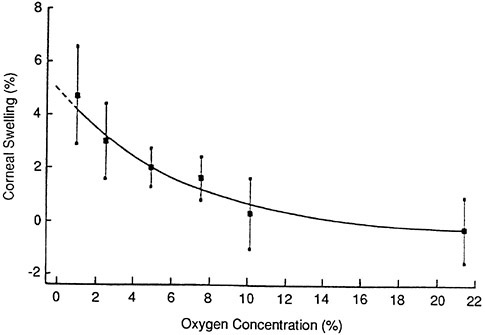
FIGURE 3 Mean corneal swelling for the group after 8 hr exposure to the various oxygen concentrations. The curve is an exponential fit. The error bars represent ±1 standard deviation. SOURCE: Holden et al. (1984). Reprinted by permission.
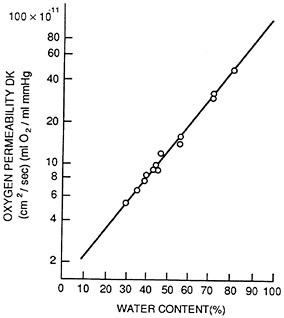
FIGURE 4 Oxygen permeability (Dk) of hydrogel lenses of various specific water contents (expressed in percentages). Dk is given in cm3 × ml O2/sec × ml × mmHg. Oxygen transmissibility was measured at a room temperature of 21°C. SOURCE: Sarver et al. (1981). Reprinted by permission.
TABLE 2 Dk/L Values for Different Water Contents and Lens Thicknesses
|
Water content |
Thickness (mm) |
Dk/L |
|
38% |
0.035 |
21.1 |
|
38% |
0.06 |
12.3 |
|
38% |
0.12 |
6.2 |
|
55% |
0.035 |
44.7 |
|
55% |
0.06 |
26.1 |
|
55% |
0.12 |
13.0 |
|
75% |
0.06 |
63.1 |
|
75% |
0.12 |
31.5 |
|
75% |
0.20 |
18.9 |
If water is lost from the lens due to dehydration, the oxygen transmissibility will decrease accordingly.
If new hydrogel materials are developed that do not depend solely on water content for oxygen diffusion, the hydrogel lenses will allow for extended wear without the present physiological problems.
With rigid gas-permeable (RGP) lenses the oxygen permeability depends on the lens material chemistry. Usually silicone and/or fluorine is added to polymethylmethacrylate to obtain gas transmission. It is possible with these materials to obtain higher oxygen transmission than with hydrogels. Because of the difficulty of measuring the Dk values of rigid materials, different values have been reported for the same material. The original values were higher than the lenses performed clinically; thus, the new lower values are more nearly correct. Table 3 shows Dk values for some common rigid materials.
Soft silicone lenses have the highest oxygen permeabilities of all materials. They have been shown to actually cause less corneal swelling when worn during sleep than if no lens is on the eye (Sweeney and Holden, 1987). With new lens designs of this material, there is promise for extended wear and use under low oxygen levels.
An environmental factor that affects the amount of oxygen reaching the cornea is the amount of oxygen in the atmosphere. At altitudes higher than sea level the amount of oxygen obviously decreases. At 5,000 feet, instead of 21 percent oxygen, there is about 18 percent; at 11,000 feet there is 14 percent and at 29,000 feet there is 7 percent (Hill, 1976; Weissman, 1980). Since even at 29,000 feet the oxygen level is about equal to that with the closed eye, one would expect an extended-wear lens to not produce excessive edema problems over the short term. The edema levels with the open eye at the high altitudes would be about the same as during sleep with the extended-wear lenses. A study by Flynn et al. (1988) did not find any
TABLE 3 Dk Values for Some Common Rigid Materials
|
Material |
Dk |
Nominal Dk |
Overnight edema (company rep.) |
|
Boston IV |
17 |
26 |
12.9 |
|
Paraperm 02+ |
18 |
39 |
|
|
Alberta N |
21 |
40 |
10.4 |
|
Paraperm EW |
27 |
56 |
11.0 |
|
Optacryl EXT |
28 |
59 |
|
|
Optacryl Z |
29 |
82 |
6.7 |
|
Equalens |
36 |
72 |
10.2 |
|
FlouroPerm |
92 |
7.6 |
|
|
Flouropolymer |
71 |
170 |
6.0 |
|
Silsight |
85 |
400 |
2.0 |
|
Sources: Brennan et al. (1986) and LaHood et al. (1988) |
|||
significant edema-related problems with simulated altitudes of 10,000 and 25,000 feet with hydrogel lens wear.
CARBON DIOXIDE
Carbon dioxide is a by-product of cornea metabolism and must be vented from under a contact lens. Only limited investigation of carbon dioxide has been carried out. It has been stated that CO2 transmissibility is 5 to 22 times greater than that for oxygen (Fatt et al., 1969; Refojo, 1979). On this assumption it has been calculated that the CO2 level under a hydrogel lens would be very low (about 3 mmHg) (Fatt, 1978). Recently, Holden et al. (1987) have shown that there is an increase in CO2 with eye closure of less than 10 minutes (Figure 5) and with the wearing of hydrogel lenses (Figure 6 ). The partial pressure of CO2 reaches approximately 50 mmHg.
CORNEAL STROMAL pH
Bonanno and Polse (1987a, 1987b) found that the pH of the corneal stroma with the open eye was 7.54. With eye closure for 20 minutes, the pH dropped to 7.39 and returned to 7.54 within 10 to 15 minutes of eye opening. With a gas mixture in a goggle consisting of 6.7 percent CO2, 7.1 percent O2, and N2, the pH dropped to 7.29. With a mixture of 5 percent CO2 and air (same as CO2 in the conjunctival vessels), the pH dropped to 7.38. This is the same as with the closed eye. With a thick hydrogel
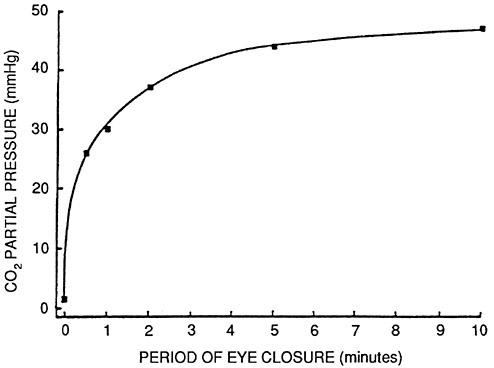
FIGURE 5 Carbon dioxide partial pressure at the anterior corneal surface immediately following short periods of eye closure. SOURCE: Holden et al. (1987). Reprinted by permission.
contact lens that provides very little O2, the pH dropped to 7.15, whereas with pure N2 in goggles, which also provides no O2, the pH dropped to only 7.34. With a mixture of 95 percent N2 and 5 percent CO2, the pH dropped to 7.16. Therefore, anoxia caused only part of the drop in pH, and CO2 buildup is required to decrease the pH, to that equivalent to wearing a tight lens.
BUBBLE FORMATION UNDER LENSES WITH PRESSURE CHANGES
Simon and Bradley (1980) have reported that decompression divers developed bubbles of gas under rigid polymethylmethacrylate (PMMA) lenses. This occurred during decompression from 45.5 meters. The bubbles caused some corneal staining. The bubbles have high surface tension due to the short radius and will indent the cornea. Under hypobaric conditions, for example, at an altitude of 11,277 meters a few small bubbles developed but did not coalesce as with the hyperbaric (diving) conditions or cause corneal staining.
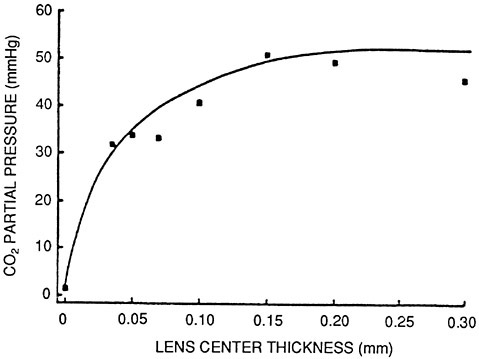
FIGURE 6 Carbon dioxide partial pressure at the anterior corneal surface immediately following 10 minutes wear of hydrogel lenses of various center thicknesses. SOURCE: Holden et al. (1987). Reprinted by permission.
NOXIOUS GASES
Very little investigation has been done on the effect of absorption and concentration of other gases into contact lens materials. Nilsson and Andersson (1982) tested the concentration of trichlorethylene and xylene in low-water-content (38 percent) and high-water-content (75 percent) lenses exposed to fumes from the air. The lenses were not on eyes. They found a concentration of trichlorethylene (after a 10-minute exposure at 700 ppm) in the low-and high-water lenses of 88 times and 170 times that in air, respectively, after 10 minutes. Under the same conditions saline absorbed about 3 times the air concentration. With xylene and longer (90-minute) exposures, the concentrations were 93 and 224 times those in the air for the two lens materials. With a 60-minute soak in saline, only 10 percent was left in the lenses.
Despite the concern, there have been no reports of clinically significant problems with fumes and the wearing of contact lenses.
REFERENCES
Bonannno, J.A., and K.A. Polse 1987a Measurement of in vivo human corneal stromal pH: open and closed eyes. Investigative Ophthalmology 28(3):522–530. 1987b Corneal acidosis during contact lens wear: effects of hypoxia and CO2. Investigative Ophthalmology 26(9):1514–1520.
Brennan, N.A., N. Efron, and B.A. Holden 1986 Oxygen permeability of hard gas permeable contact lens materials. Clinical and Experimental Optometry 69(3):82–89.
Cuklanz, H.D., and R.M. Hill 1969 Oxygen requirements of contact lens systems. American Journal of Optometry 46(9):662.
Efron, E., and N.A. Brennan 1987 In search of the critical oxygen requirement of the cornea. Contax.
Fatt, I. 1969 Oxygen tension under a contact lens during blinking. American Journal of Optometry 46(9):654. 1978 Gas transmission properties of soft contact lenses. Pp. 108–109 in M. Ruben ed. Soft Contact Lenses: Clinical and Applied Technology. New York : John Wiley & Sons.
Fatt, I., and R.M. Hill 1970 Oxygen tension under a contact lens during blinking—a comparison of theory and experimental observation. American Journal of Optometry 47(1):50–55.
Fatt, I., M.T. Bieber, and S.D. Pye 1969 Steady state distribution of oxygen and carbon dioxide in the in vivo cornea of an eye covered by a gas-permeable contact lens. American Journal of Optometry 64(3):14.
Flynn, W.J., et al. 1988 Soft contact lens wear at altitude: effects of hypoxia. Aviation, Space, and Environmental Medicine 59(1):44–48.
Hill, R.M. 1976 Perils of the pupil. International Contact Lens Clinic 3(3):48–49.
Hill, R.M., and I. Fatt 1963 Oxygen uptake from a reservoir of limited volume by the human cornea in vivo. Science 142:1295.
Hill, R.M., and T.F. Mauger 1980 Oxygen update: hydrophilics. International Contact Lens Clinic 7(5):47–49.
Holden, B.A., and G.W. Mertz 1984 Critical oxygen levels to avoid corneal edema for daily and extended wear contact lenses. Investigative Ophthalmology 25(10):1161–1167.
Holden, B.A., D.F. Sweeney, and G. Sanderson 1984 The minimum precorneal oxygen tension to avoid corneal edema. Investigative Ophthalmology 25(4):476–480.
Holden, B.A., R. Ross, and J. Jenkins 1987 Hydrogel contact lenses impede carbon dioxide efflux from the human cornea. Current Eye Research 6(11):1283.
LaHood, D., D.F. Sweeney, and B.A. Holden 1988 Overnight corneal edema with hydrogel, rigid gas permeable and silicone elastomer contact lenses. International Contact Lens Clinic 15(5):149–153.
Larke, J.R., S.T. Parrish, and C.G. Wigham 1981 Apparent human corneal oxygen uptake rate. American Journal of Optometry 58(10):803–805.
Nilsson S.E.G., and L. Andersson 1982 The use of contact lenses in environments with organic solvents, acids or alkalis. Acta Ophthalmologica 60:599–608.
Polse, K.A. 1979 Tear flow under hydrogel contact lenses. Investigative Ophthalmology 18(4):409–413.
Refojo, M.F. 1979 Mechanism of gas transport through contact lenses. Journal of the American Optometric Association 50:285–287.
Sarver, M.D., et al. 1981 Corneal edema with hydrogel lenses and eye closure: effect of oxygen transmissibility. American Journal of Optometry 58(5):386–392.
Simon, D.R., and M.E. Bradley 1980 Adverse effects of contact lens wear during decompression. Journal of the American Medical Association 244:1213–1214.
Sweeney, D.F., and B.A. Holden 1987 Silicone elastomer lens wear induces less overnight corneal edema than sleep without lens wear. Current Eye Research 6(12):1391.
Wagner, L., K. Polse, and R. Mandell 1980 Tear pumping and edema with soft contact lenses. Investigative Ophthalmology 19(11):1397–1400.
Weissman, B.A. 1980 Predicted changes in tear layer oxygen. International Contact Lens Clinic 7(5):41–44.











