
5
Preventive Interventions
The research on bullying prevention programming has increased considerably over the past 2 decades, which is likely due in part to the growing awareness of bullying as a public health problem that impacts individual youth as well as the broader social environment. Furthermore, the enactment of bullying-related laws and policies in all 50 states has drawn increased focus on prevention programming. In fact, many state policies require some type of professional development for staff or prevention programming related to bullying (Hatzenbuehler et al., 2015; Stuart-Cassel et al., 2011). Despite this growing interest in and demand for bullying prevention programming, there have been relatively few randomized controlled trials (RCTs) testing the efficacy or effectiveness of programs specifically designed to reduce or prevent the onset of bullying or offset its consequences on children and youth (Bradshaw, 2015; Jiménez-Barbero et al. 2016). Moreover, the much larger body and longer line of research focused on aggression, violence, and delinquency prevention has only recently begun to explore program impacts specific to bullying. The focus of that research has typically been on broader concepts, such as aggression, violence, delinquency, externalizing problems, etc. Therefore, it is quite possible that there are several violence or aggression prevention programs that have substantial effects on bullying, but there is currently too little data available from most violence prevention studies that employ RCT designs to formulate a conclusion regarding impacts on bullying specifically (Bradshaw, 2015).
In this chapter, the committee summarizes the current status of bullying prevention programming, while acknowledging both gaps in the extant literature and opportunities for future research. The committee first focuses
more narrowly on bullying prevention and intervention programming for which there are data specifically on bullying behaviors; greater emphasis is placed on RCTs, as compared to nonexperimental, correlational, or descriptive studies. The committee then considers the broader literature on other youth-focused violence prevention and intervention programming, with particular attention to potential conceptual or measurement overlap with bullying, since such models may hold promise for reducing rates or effects of bullying (Bradshaw, 2015; Hawkins et al. 2015). Although the committee was intentionally inclusive of the larger body of prevention programming literature, it acknowledges the caveats of such a broad focus, as findings from other violence prevention programs may not always generalize to bullying-specific outcomes (e.g., Espelage et al., 2013). Nevertheless, this review is not intended to be an exhaustive list of all evidence-based approaches to bullying or youth violence prevention; rather, the committee highlights particular models and frameworks for which there is a strong or emerging line of RCT studies suggesting promise for preventing or offsetting the consequences of bullying.
In an effort to organize the vast and somewhat disparate lines of prevention literature, the committee adopted the National Research Council’s public health model of mental health intervention (Institute of Medicine, 1994) as a framework for conceptualizing the various programs and models across increasing levels of intensity (see Figure 5-1).
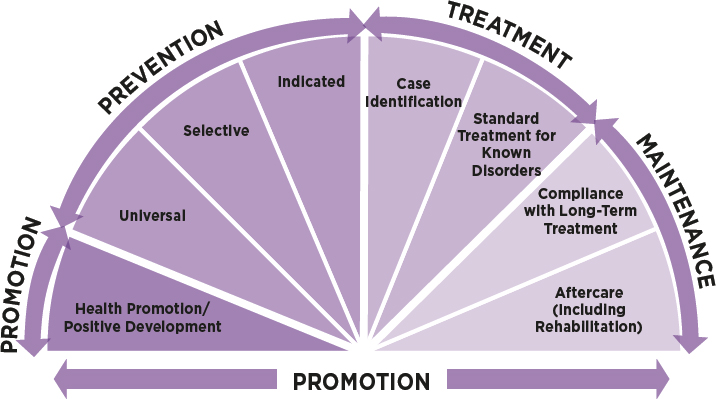
SOURCE: Adapted from Institute of Medicine (1994, Fig. 2.1, p. 23).
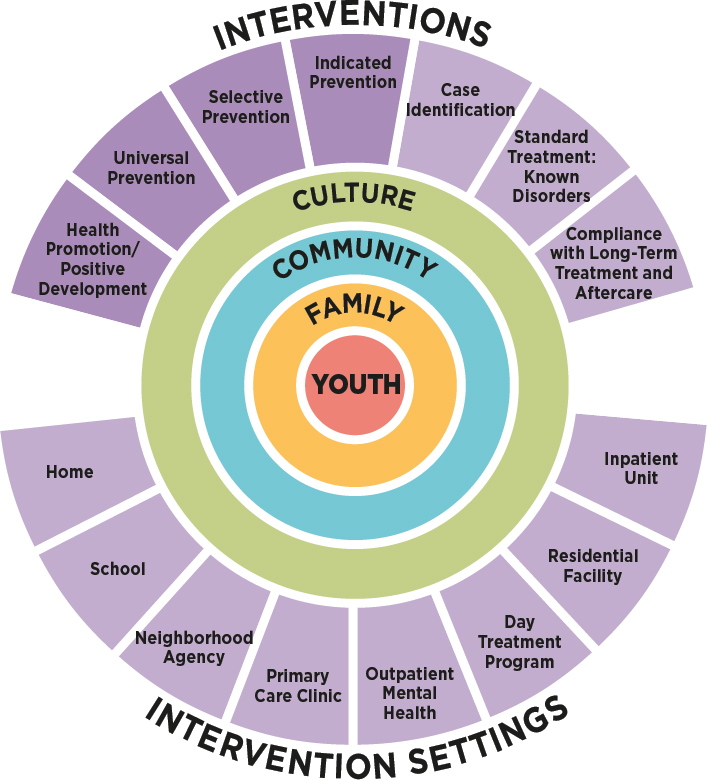
SOURCE: Adapted from National Research Council and Institute of Medicine (2009, Fig. 4-1, p. 73).
This model includes three levels of prevention programming (i.e., universal, selective, and indicated), which are preceded by promotion-focused programming and followed by treatment and maintenance (National Research Council and Institute of Medicine, 2009). Mental health promotion has been recognized as a key component of the mental health intervention continuum (National Research Council and Institute of Medicine, 2009). Although prevention programming can occur in multiple settings and ecological contexts (see Figure 5-2; also Espelage and Swearer, 2004; Swearer
et al., 2010; Weisz et al., 2005), the majority of research has been conducted within schools. As a result, the committee made an effort to also provide examples of programs that occur in settings other than school, even when the literature base was thinner as it relates to bullying-specific programming and/or outcomes. After summarizing various research-based prevention frameworks and programs, the committee concludes by highlighting lessons learned from the extant research as it relates to critical features of bullying prevention programming and identifying future research directions related to bullying prevention programming.
MULTI-TIERED PREVENTION FRAMEWORK
An increasingly common approach to the prevention of emotional and behavioral disorders is the three-tiered public health model that includes universal, selective, and indicated preventive interventions, as illustrated in Figure 5-1 (Institute of Medicine, 1994; National Research Council and Institute of Medicine, 2009; Weisz et al., 2005). Similar frameworks have been proposed or articulated to conceptualize a multi-tiered system of supports (for a review, see Batsche, 2014). Although this continuum of preventive interventions can be applied to many behavioral, educational, mental health, and physical health problems, this report considers it primarily through the lens of bullying prevention among youth.
The Three Tiers
Specifically, universal prevention programs are aimed at reducing risks and strengthening skills for all youth within a defined community or school setting. Through universal programs, all members of the target population are exposed to the intervention regardless of risk for bullying. Using universal prevention approaches, a set of activities may be established that offers benefits to all individuals within that setting (e.g., school). Examples of universal or Tier 1 preventive interventions include social-emotional lessons that are used in the classroom, behavioral expectations taught by teachers, counselors coming into the classroom to model strategies for responding to or reporting bullying, and holding classroom meetings among students and teachers to discuss emotionally relevant issues related to bullying or equity. Universal interventions could also include guidelines for the use of digital media, such as youth’s use of social network sites.
Most of the bullying prevention programs that have been evaluated with RCT designs have employed a universal approach to prevention (Ttofi and Farrington, 2011; Jiménez Barbero et al., 2016). Although universal bullying prevention programs are typically aimed at having effects on youth, they may also yield benefits for the individuals implementing the
programs. For example, recent findings from a RCT of a social–emotional learning and behavior management program indicated that the program substantially affected the teachers who implemented the program, as well as affecting the students (Domitrovich et al., 2016). Similarly positive effects were observed in a randomized trial of a schoolwide Positive Behavior Support model, where implementation of the model demonstrated significant impacts on the staff members’ perceptions of school climate (Bradshaw et al., 2009a). Consistent with the social-ecological model, these effects may be either direct—through the professional development provided to the teachers—or indirect through the improved behavior and enhanced organizational context of the setting in which the program is implemented. These types of secondary impacts on the broader school or community environment also likely occur in universal bullying prevention programs, many of which are intended to reduce bullying in conjunction with improving school climate (Bradshaw, 2013).
Most school-based bullying prevention programs would fall under the universal category of largely preventive interventions, with limited articulation of specific programs, activities, or supports for students not responding adequately to the universal model. Even if the programs focus on the whole school or climate/culture changes, they often take the perspective that a universal approach is the most important and potentially most effective intervention because all children can benefit from attempts to enhance school climate, change attitudes or awareness about bullying, reduce aggressive behavior, or improve related social skills or behavior. Furthermore, some universal programs follow the assumption that all students are considered to be at risk at some level for bullying behavior, either as perpetrators, targets, or bystanders (Rigby and Slee, 2008). In fact, there is a growing recognition that universal prevention programs do not equally benefit all individuals; rather, evidence is emerging that universal prevention programs may actually be more effective for higher risk students than those traditionally conceptualized as low risk (Bradshaw et al., 2015; Eron et al., 2002; Kellam et al., 1994). As a result, there is a growing trend in prevention research to explicitly examine variation in responsiveness to universal prevention programs in order to better understand which youth may be most affected by a particular model (Kellam et al., 1994; Lanza and Rhoades, 2013). This may also improve understanding of why some effect sizes of universal prevention programs are relatively modest when they are averaged across a large population, as a broader population may have a relatively low base rate for engaging in the behavior (Biglan et al., 2015). On the other hand, investing in prevention on a national level has the potential to produce significant and meaningful behavior change for larger populations of youth across a broad array of outcomes, not just outcomes related to
bullying behavior (Biglan et al., 2015; Institute of Medicine and National Research Council, 2015).
The next level of the tiered prevention model is referred to as selective preventive interventions. These may either target youth who are at risk for engaging in bullying or target youth at risk of being bullied. Such programs may include more intensive social-emotional skills training, coping skills, or de-escalation approaches for youth who are involved in bullying. Consistent with a response-to-intervention framework, these Tier 2 approaches are employed to meet the needs of youth who have not responded adequately to the universal preventive intervention (National Research Council and Institute of Medicine, 2009).
The third tier includes indicated preventive interventions, which are typically tailored to meet the youth’s needs and are of greater intensity as compared to the two previous levels of prevention. Indicated interventions incorporate more intensive supports and activities for those who are already displaying bullying behavior or have a history of being bullied and are showing early signs of behavioral, academic, or mental health consequences. The supports are usually tailored to meet the needs of the students demonstrating negative effects of bullying (Espelage and Swearer, 2008); they typically address mental and behavioral health concerns, often by including the youth’s family. Such programs may also leverage expertise and involvement of teachers, education support professionals, school resource officers, families, health care professionals, and community members, thereby attempting to support the participating youth across multiple ecological levels. While a number of selective and indicated programs have demonstrated efficacy for a range of youth behavioral and mental health problems (for a review see National Research Council and Institute of Medicine, 2009), there has been considerably less research on selective and indicated prevention programs specific to bullying (Swearer et al., 2014).
Integrating Prevention Programs across the Tiers
Consistent with the public health approach to prevention (National Research Council and Institute of Medicine, 2009) and calls for multi-tier or multidisciplinary approaches to prevention, there is an increasing interest in layering components “on top of” or in combination with the universal intervention to address factors that may place youth at risk for being targets or perpetrators of bullying (universal plus targeted interventions). These combined programs often attempt to address at the universal level such factors as social skill development, social-emotional learning or self-regulation, which are intended to also reduce the chances that youth would engage in bullying or reduce the risk of further being bullied (Bradshaw, 2013, 2015; Merrell et al., 2008; Ttofi and Farrington, 2011; Vreeman and
Carroll, 2007). These combined programs are often characterized as universal, whole school, or climate/culture changing programs that may have additional “benefits” for perpetrators or targets (e.g., help them be more effective in coping with the stress of bullying). However, few have easily identifiable components that specifically target youth at risk for involvement in bullying behavior or those already identified as perpetrators or targets. Therefore much of what is currently known about bullying prevention derives from studies of universal programs, with limited research on selective and indicated models for prevention.
Current research is limited in its ability to specifically tease out the effects of targeted elements embedded in whole-school universal programs (Bradshaw, 2015; Ttofi and Farrington, 2011). For example, evaluators have not been able to assess whether it is the universal or targeted components (or the combination of the two) that leads to reductions in bullying behavior or improvements in social-emotional skills (Ttofi and Farrington, 2011). In fact, few of the truly multi-tiered programs have been evaluated using randomized, controlled esperimental designs to determine whether they are effective or lead to sustained behavior change. Moreover, once a child or youth is identified as a target or a perpetrator of bullying, the individual is often referred to mental health or behavioral health services providers in the community—in part because few school-based mental health professionals are available to provide these specialized services (Swearer et al., 2014).
In summary, despite calls for a layered public health approach to bullying prevention or calls for multicomponent, multilevel programs (Leff and Waasdorp, 2013), few studies of school-based bullying prevention programs have simultaneously evaluated both universal and targeted components (Bradshaw, 2015). Although many researchers encourage the use of a multi-tiered approach to address bullying, and there is conceptual research supporting the full integration of preventive interventions (Bradshaw, 2013, 2015; Espelage and Swearer, 2008; Hawley and Williford, 2015; Hong and Espelage, 2012; Swearer et al., 2012), relatively few large-scale RCT studies have examined the combined and tier-specific effects of multi-tiered programs on bullying. Yet, integrating the nested levels of support into a coherent, tiered framework could also reduce burden and increase efficiency of implementation (Bradshaw et al., 2014a; Domitrovich et al., 2010; Sugai and Horner, 2006).
PREVENTION PROGRAMS SPECIFICALLY IMPLEMENTED TO REDUCE BULLYING AND RELATED BEHAVIOR PROBLEMS
The sections that follow focus on the available efficacy and effectiveness research that has examined different bullying prevention programs, the vast majority of which have been implemented at the universal level and within schools. The committee first considers the evidence for the effectiveness of universal programs, many of which are whole-school efforts that may include some elements directed to youth at risk for bullying or those already engaged in bullying behaviors.1 The committee also reviews the effectiveness of specific selective or indicated prevention programs, many of which were designed more broadly for youth with behavioral or mental health problems, rather than specifically for bullying.
The committee considered the broader literature on programs aimed at reducing youth aggressive behavior and those aimed at improving emotional and behavioral problems among youth. While most of these programs were not originally developed to address bullying behavior specifically, one may still learn much from them about means to reduce bullying-related behavior, or they may provide clues about how to improve resilience, social competence, or problem-solving skills that may lead to reductions in bullying perpetration or being bullied. In some instances, the committee has drawn
___________________
1 Clinicians and policy makers define efficacy trials as trials that determine whether “an intervention produces expected results under ideal circumstances” and effectiveness trials as trials that “measure the degree of beneficial effect under ‘real world’ clinical settings” (Gartlehner et al., 2006).
upon literature from related fields, such as trauma exposure or research on how families can promote emotional resilience to being a target of bullying (Bowes et al., 2010). Few of these studies, however, have assessed or examined the impact of these interventions on behaviors specific to bullying. Rather, they may assess behaviors such as fighting, threats, violence, aggressive, or delinquent behavior. If one takes the position that most bullying can be characterized as aggressive behavior but not all aggressive or violent behavior meets the narrower definition of bullying (Farrington and Ttofi, 2011; Finkelhor et al., 2012; Leff and Waasdorp, 2013), then perhaps there are lessons to learn from interventions that have shown reductions in aggression and violence or improvements in social skills, even if bullying behavior was not the primary focus of the intervention. The same thinking applies to studies of peer victimization in that while being bullied may be characterized as a form of victimization, not all victimization by peers would be characterized as bullying, particularly with respect to the criteria of repeated targeting or a power imbalance (Finkelhor et al., 2012).
Another reason the committee has considered the broader violenceprevention literature is that bullying often co-occurs with other behavioral and mental health problems, including aggression and delinquent behaviors (Bradshaw et al., 2013a; Swearer et al., 2012), and the risk factors targeted through preventive interventions are often interrelated. For example,
aggressive youth are more likely to be rejected by their peers, to have associated academic problems (Nansel et al., 2003), or to experience higher rates of family discord or maltreatment (Shields and Cicchetti, 2001). Further, many preventive interventions seek to enhance positive or prosocial behaviors or improve social competence, in addition to reducing negative behaviors such as aggression and fighting (Embry et al., 1996; Flannery et al., 2003).
For example, a meta-analysis of school-based mental health promotion programs found that they can improve social-emotional skills, prosocial norms, school bonding, and positive social behavior, as well as result in reduced problem behaviors, such as aggression, substance use, and internalizing symptoms (Durlak et al., 2007; Durlak et al., 2011). An improvement in competence and social problem-solving skills may lead to reductions in bullying perpetration even if that was not the intended outcome of the intervention. Other studies have demonstrated improvements in youth coping skills and stress management (Kraag et al., 2006), which can be helpful to children who are bullied even if such children were not the original population targeted by the intervention. In summary, many school and community-based programs were not originally designed to specifically reduce bullying, but because they target related behaviors, they may provide valuable lessons that can inform efforts related to bullying prevention.
Summary of the Available Meta-Analyses
A number of recent meta-analyses have been conducted in an effort to identify the most effective and promising approaches within the field of bullying prevention; for a review of the meta-analyses see Ttofi and colleagues (2014). The most comprehensive review conducted to date was by Ttofi and Farrington (2011), who applied the Campbell Systematic Review procedures in reviewing 44 rigorous program evaluations and RCTs. The majority of these studies were conducted outside the United States or Canada (66%), and over a third of the programs were based in part on the work of Olweus (1993). Ttofi and Farrington (2011) found that the programs, on average, were associated with a 20-23 percent decrease in perpetration of bullying, and a 17-20 percent decrease in being bullied, as illustrated in Figures 5-3 and 5-4.2
As in other reviews and meta-analyses (Bradshaw, 2015; Leff and Waasdorp, 2013), Farrington and Ttofi (2009) concluded that in general the
___________________
2 The committee includes details of studies where possible, in particular if the study employed a RCT design and where effect sizes are reported or control groups were used. We encourage the reader to refer to the original studies for additional details about study design, population, measurement, variables included in analyses, etc.
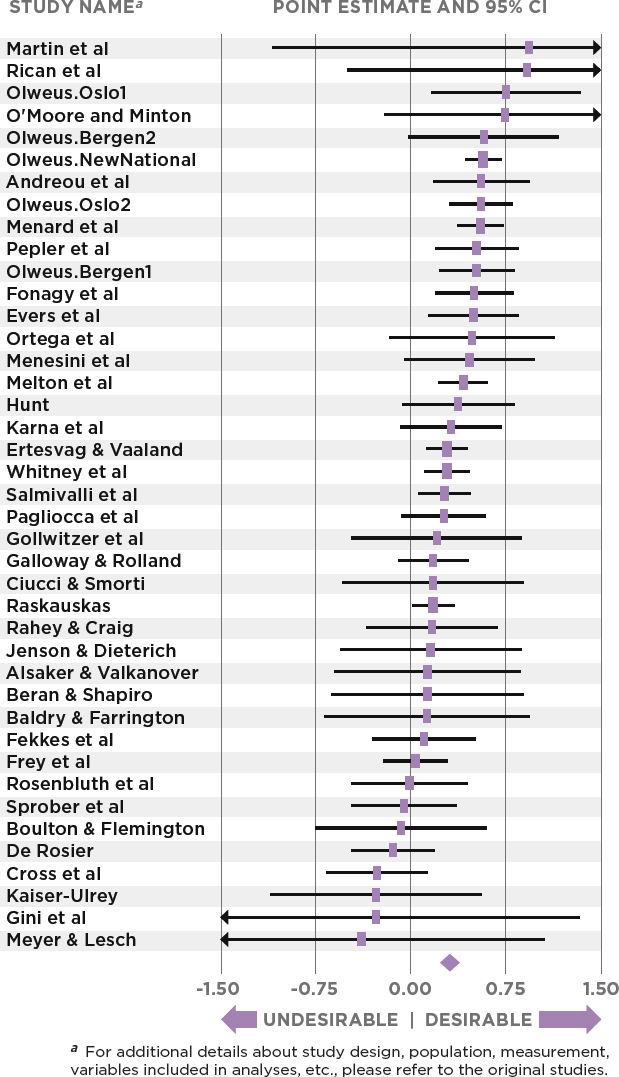
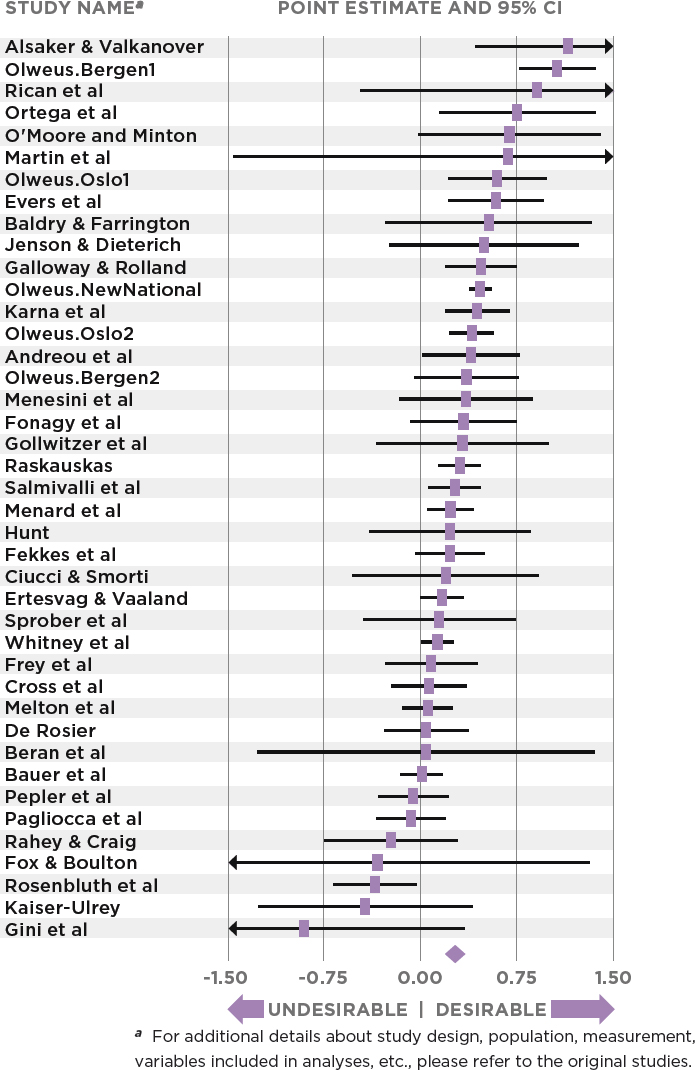
most effective programs are multicomponent, schoolwide programs that reduce bullying and aggression across a variety of settings. However, as noted previously, these multicomponent programs are not always multi-tiered in the context of the public health model; rather, they may have multiple complementary program elements that all focus on universal prevention, such as a combination of a whole-school climate strategy coupled with a curriculum to prevent bullying or related behaviors. Furthermore, the designs of the studies precluded the researchers from isolating which program elements accounted for the program impacts. Nevertheless, Farrington and Ttofi (2009) concluded that parent training, improved playground supervision, disciplinary methods, school conferences, videos, information for parents, classroom rules, and classroom management were program components associated with a decrease in students being bullied.
The whole-school bullying prevention programs (mostly based on or modeled after the extensively studied Olweus Bullying Prevention Program model, which aims at reducing bullying through components at multiple levels) also generally demonstrated positive effects, particularly in schools with more positive student-teacher relationships (Richard et al., 2012). In general, significant intervention effects have been demonstrated more often for programs implemented in Europe (Richard et al., 2012) and Scandinavian countries (Farrington and Ttofi, 2009; Salmivalli, 2010) than in the United States (also see Bradshaw, 2015). Some researchers and practitioners have suggested that interventions implemented outside the United States may be more successful because they involve more homogeneous student samples in schools that are more committed to implementing programs as intended (Evans et al., 2014), compared with student samples and schools’ commitment in the United States. Competing demands on student and teacher time, such as standardized testing, also limit U.S. teachers’ perceived ability to focus on social-emotional and behavioral activities, as compared with traditional academic content. The challenges in designing and delivering effective bullying prevention programs in the United States may also include the greater social and economic complexities of U.S. school populations, including greater income disparities and racial/ethnic heterogeneity.
The meta-analyses, most notably the Ttofi and Farrington (2011) review, noted variation in program effects based on study design, as has been shown for most such intervention programs. For example, large-scale effectiveness studies (i.e., studies of taking an intervention program to scale) did not produce effects as strong as those in more tightly controlled efficacy studies, where the program is often administered with greater support and researcher influence (Bradshaw, 2015; Ttofi and Farrington, 2011). Similarly, the effects generally were stronger in the non-RCT designs than in the RCTs, suggesting that the more rigorous the study design, the smaller the effect sizes (Farrington and Ttofi, 2009). Moreover, as has been shown in
several other studies across multiple fields (e.g., Domitrovich et al., 2008), poor implementation fidelity has been linked with weaker program outcomes (also see Durlak et al., 2011).
Another important finding from the Ttofi and Farrington review was that, generally speaking, there are more school-based bullying prevention programs that involve middle-school youth than those that target youth of high school age. Of the programs that have been evaluated with RCT designs, the observed effects were generally larger for older youth (ages 11-14) than for younger children (younger than age 10) (Farrington and Ttofi, 2009; Ttofi and Farrington, 2011). However, this effect has not been consistent across all programs and all studies, as there is compelling developmental research suggesting that the earlier one intervenes to prevent behavior problems, the more effective the intervention is (Kellam et al., 1994; Waasdorp et al., 2012). Unpacking this finding is likely to be complicated because different programs are often used at different age ranges, thereby confounding the child’s age with the program used. However, more recently, some programs that were originally developed for a particular age group have been adapted for youth of a different age range (e.g., Promoting Alternative Thinking Strategies, Second Step, Coping Power; Olweus Bullying Prevention Program). Implementations of these programs span multiple age groups, with specific curricular or program activities that are developmentally appropriate for the target population (e.g., to address different developmental needs for a third grader than for an eighth grader).
Other meta-analyses of school-based bullying intervention programs have not been as positive as the Ttofi and Farrington (2011) review (e.g., Merrell et al., 2008; Vreeman and Carroll, 2007). Some of these mixed findings may be due to different inclusion criteria, such as where the study was conducted (e.g., in the United States or Europe) or who conducted it (i.e., the program developer or an external evaluator). For example, Merrell and colleagues (2008) reviewed 16 studies of over 15,386 kindergarten through grade 12 (K-12) students in six different countries from 1980 through 2004. They concluded that the majority of outcomes were neither positive nor negative and generally lacked statistical significance one way or the other (they found a meaningful positive average effect on bullying for about one-third of all outcomes). They further concluded that programs are much more likely to show effects on attitudes, self-perceptions, and knowledge than on bullying behavior. Only one of the reviewed studies specifically included an intervention for at-risk students; a program that assigned social workers to the primary school building to work with students at risk for perpetrating or being targets of bullying (Bagley and Pritchard, 1998). Bagley and Pritchard (1998) assessed student self-reports of bullying incidents and showed significant declines in bullying among students who received intervention services from social workers. Merrell and his col-
leagues (2008) did not weight the 16 studies in the meta-analysis for sample size, degree of experimental rigor, or threats to validity when they computed effect sizes within the individual research studies. Overall, however, they concluded that while some intervention studies had positive outcomes, these were mostly for attitudes and knowledge rather than improving (lessening the frequency of) youth self-reports of being perpetrators or targets of bullying (Merrell et al., 2008; Smith et al., 2004).
Vreeman and Carroll (2007) also conducted a systematic review of bullying preventive interventions, some of which combined programs across the tiers. They found that whole-school approaches with teacher training or individual counseling did better than curricular-only approaches. Of the 26 studies that met their inclusion criteria, only four included targeted interventions involving social and behavioral skills groups for children involved in bullying as perpetrators (Fast et al., 2003; Meyer and Lesch, 2000) and two targeted youth who were victims of bullying (DeRosier, 2004; Tierney and Dowd, 2000). According to Vreeman and Carroll (2007), three of the four studies focused on youth in middle school (sixth through eighth grade) and one examined third grade students. The only social skills training intervention that showed clear reductions in bullying was the study of third grade students. The other three studies of older youth produced mixed results.
Another more recent meta-analysis of bullying prevention programs by Jiménez-Barbero and colleagues (2016) examined a range of effects of 14 “anti-bullying” programs tested through RCTs, comprising 30,934 adolescents ages 10-16. All studies were published between 2000 and 2013. They examined not only bullying frequency (ES = 0.12) and victimization frequency (ES = 0.09), but also attitudes favoring bullying or school violence (ES = 0.18), attitudes against bullying or school violence (ES = 0.06), and school climate (ES = 0.03). See details of the individual studies below in Figure 5-5. This study was considerably smaller in scale than the Ttofi and Farrington (2011) meta-analysis, in large part because of stricter inclusion criteria. Furthermore, on average, these effect sizes were smaller than observed in the Ttofi and Farrington (2011) study. Because of the smaller sample size, it is difficult to formulate conclusions based on specific components (e.g., family, teacher) or youth subgroups (e.g., age of students). Taken together, the meta-analyses provide evidence that the effect sizes of universal programs are relatively modest. Yet these effects are averaged across a full population of youth; selective and indicated prevention approaches, which focus on youth more directly involved in bullying, will likely yield larger effect sizes, as has been seen in other studies of violence prevention programming (discussed later in this chapter).
In contrast to the somewhat mixed findings on interventions specifically for bullying prevention, the larger body of universal youth violence preven-
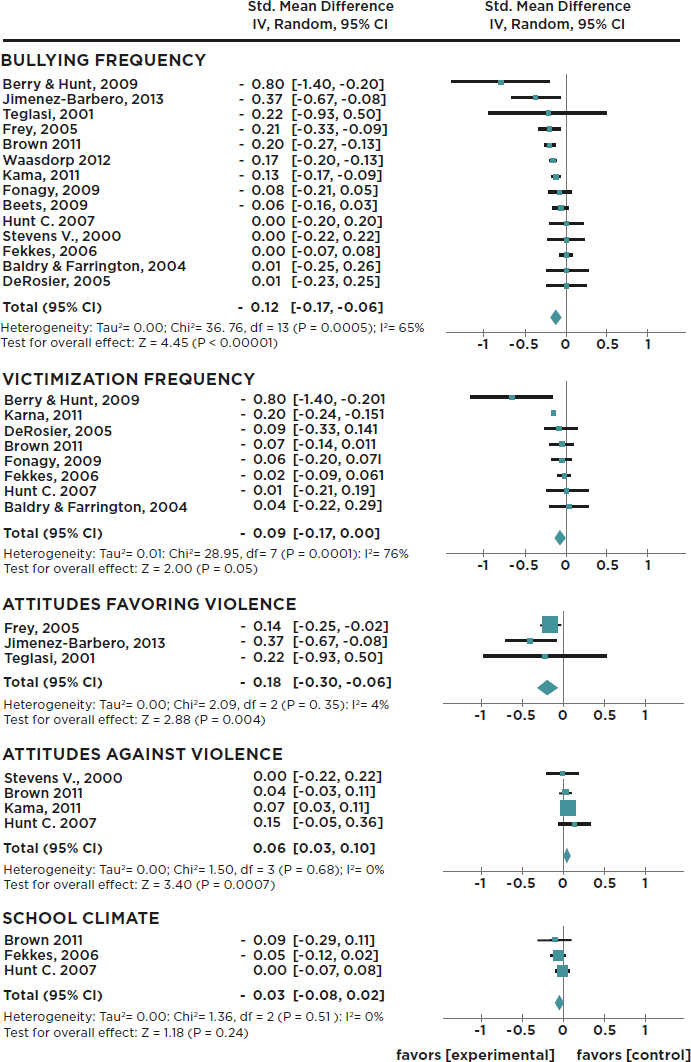
NOTE: For additional details about study design, population, measurement, variables included in analyses, etc., please refer to the original studies.
SOURCE: Adapted from Jiménez-Barbero et al. (2016, Fig. 2, p. 171).
tion programming has generally had more favorable results, particularly for preschool and elementary school children (Sawyer et al., 2015; Wilson and Lipsey, 2007). Systematic reviews and meta-analyses of school-based violence prevention programs (most that did not specifically address bullying behaviors) have shown many to be effective at reducing aggressive behavior and violence (Botvin et al., 2006; Durlak et al., 2011; Hahn et al., 2007; Mytton et al., 2002). Whereas some of the reviews of programs focused on bullying have reported greater effects for older students in middle or secondary schools versus students in primary schools (Mytton et al., 2002; Ttofi and Farrington, 2011), the programs focused on aggression and social competence have shown greater effects for younger children (Kärnä et al., 2011a). One factor may be variations in focus, such as reviews that cover secondary prevention trials for those at risk for aggression and violence (Mytton et al., 2002) versus reviews that include universal and whole school violence prevention programs (Hahn et al., 2007). For example, a review of violence prevention programs by Limbos and colleagues (2007) found that about one-half of 41 intervention studies showed positive effects, with indicated interventions for youth already engaged in violent behavior being more effective than universal or selective interventions.
Another comprehensive meta-review of 25 years of meta-analyses and systematic reviews of youth violence prevention programs concluded that most interventions demonstrate moderate program effects, with programs targeting family factors showing marginally larger effects compared to those that did not (Matjasko et al., 2012). Strength of evidence was rated as small, moderate, or strong by the authors using data on reported effect sizes. This meta-review suggested that studies consistently reported larger effect sizes for reduction of youth violent behavior for programs that targeted selected and indicated populations of youth versus universal prevention. The authors also found that programs with a cognitive-behavioral component tended to have larger effect sizes than those without that component or with only a behavioral component (Matjasko et al., 2012). These findings are generally consistent with a recent meta-analysis by Barnes and colleagues (2014), who found that school-based cognitive behavioral interventions were effective (mean ES = −0.23) on reducing aggressive behavior, especially those delivered universally compared with those provided in small group settings (Barnes et al., 2014).
Examples of Universal Multicomponent Prevention Programs to Address Bullying or Related Behavior
As noted above, many schoolwide bullying prevention programs include multiple components, both within and across the three prevention tiers. One such program is the Olweus Bullying Prevention Program (Olweus,
2005), which is also the most extensively studied bullying prevention program. It aims to reduce bullying through components at multiple levels, including schoolwide components; classroom activities and meetings; targeted interventions for individuals identified as perpetrators or targets; and activities aimed to increase involvement by parents, mental health workers, and others. Some studies of the Olweus Bullying Prevention Program have reported significant reductions in students’ reports of bullying and antisocial behaviors (e.g., fighting, truancy) and improvements in school climate (Olweus et al., 1999). However, some smaller-scale studies of this model produced mixed results (e.g., Hanewinkel, 2004). Although other derivations of Olweus’s model also have demonstrated promise at reducing bullying in North America (e.g., Pepler et al., 2004), these programs were generally more effective in Europe. Farrington and Ttofi (2009) found that programs that were conceptually based on the Olweus Bullying Prevention Program were the most effective, compared to the other programs examined (OR = 1.50 versus OR = 1.31, p = .011).
Another multicomponent and multi-tiered prevention model is Positive Behavioral Interventions and Supports (PBIS) (Sugai and Horner, 2006; see also Walker et al., 1996). PBIS aims to prevent disruptive behaviors and promote a positive school climate through setting-level change, in order to prevent student behavior problems systematically and consistently. The model draws upon behavioral, social learning, organizational, and positive youth development theories and promotes strategies that can be used by all staff consistently across all school contexts (Lewis and Sugai, 1999; Lindsley, 1992; Sugai et al., 2002). Through PBIS, staff and students work together to create a schoolwide program that clearly articulates positive behavioral expectations, provides incentives to students meeting these expectations, promotes positive student-staff interactions, and encourages data-based decision making by staff and administrators. The model aims to alter the school environment by creating both improved systems (e.g., discipline, reinforcement, and data management systems) and procedures (e.g., collection of office referral data, training, data-based decision making) in order to promote positive change in student and teacher behaviors (Kutash et al., 2006; Sugai and Horner, 2006). The PBIS model also emphasizes coaching to tailor the implementation process to fit the culture and context of the school. The PBIS framework acknowledges that there is no one-size-fits-all program or model, therefore, coaches work with the schools to collect data in order to identify needs and both local challenges and resources. They subsequently help the school choose the most suitable program to be integrated within the PBIS framework, and they provide support to staff to optimize implementation fidelity.
The PBIS model follows a multi-tiered prevention approach (Institute of Medicine, 1994; National Research Council and Institute of Medicine,
2009), whereby Tier 2 (selective/targeted) and Tier 3 (indicated) programs and supports are implemented to complement the Tier 1 (universal) components (Sugai and Horner, 2006; Walker et al., 1996). Recent randomized effectiveness trials of PBIS, largely focused on the universal, Tier 1 elements, have reported significant effects on bullying and peer rejection (effect sizes ranging from 0.11 to 0.14; see Bradshaw, 2015; Waasdorp et al., 2012), as well as school climate (effect sizes from 0.16 to 0.29; see Bradshaw et al., 2008; Horner et al., 2009), and discipline problems (effect sizes from 0.11 to 0.27; see Bradshaw et al., 2010, 2012, 2015). Other significant effects have been reductions in suspensions and office referrals (ES = 0.27; see Bradshaw et al., 2008, 2009a, 2010; Horner et al., 2009; Waasdorp et al., 2012). Another randomized trial of PBIS combining Tier 1 and 2 supports in elementary schools also demonstrated significant improvements, relative to Tier 1 only, on teacher and student behaviors such as special education usage, need for advanced tier supports, and teacher efficacy to manage student behavior problems (Bradshaw et. al., 2012). An ongoing RCT of PBIS in 58 high schools, which combines other programs at Tiers 2 and 3, is currently under way; the preliminary findings from this trial suggest positive effects on bullying, violence, school climate, and substance use (Bradshaw et al., 2014b).
The KiVa Antibullying Program is another schoolwide, multicomponent program that has demonstrated promising effects. It has been implemented nationally in Finland for students in grades 1 through 9. Its universal elements include activities designed to increase bystander empathy and efficacy, teacher training, and more-targeted strategies for students at risk for or engaged in bullying as perpetrators or victims. It provides classroom training and materials to promote open discussions between teachers and students, peer support for students who are bullied, training for school staff in disciplinary strategies, and informational materials for families to prevent and appropriately respond to bullying. Computer games are also used to help students practice bullying prevention skills.
In their nonrandomized national trial, Kärnä and colleagues (2011a, 2011b) showed that after 9 months of implementation, students in KiVa schools reported lower rates of bullying behavior compared to students in non-intervention control schools. Specifically, victimization rates decreased with age from grade 1 (25.9%) to grade 9 (9.3%), with the largest decrease occurring between grades 1 and 6. Compared to controls, students in the KiVa program reported lower rates of being targeted for bullying (OR = 1.22; 95% CI [1.19, 1.24]) and perpetration of bullying (OR = 1.18; 95% CI [1.15, 1.21]).
Previous evaluations of the KiVa Program have also found the greatest program effects for younger elementary age students (grades 1-6) and smaller effects for middle-school age children (grades 7-9). Generally, pro-
gram effects increased through grade 4 but steadily declined from that point forward. Specifically, KiVa has demonstrated significant impacts on being a perpetrator or a target of bullying behavior among students in grades 4-6 (effect sizes from 0.03 to 0.33; see Kärnä, et al., 2011a, 2011b), as well as for youth in grades 1-9 (odds ratios from 0.46 to 0.79; see Garandeau et al., 2014). In one evaluation of the KiVa Program, Veenstra and colleagues (2014) showed that for fourth to sixth grade students, their perception of teacher efficacy in decreasing bullying was associated with lower levels of peer-reported bullying. They argued that teachers play an important role in anti-bullying programs and should be included as targets of intervention. Ahtola et al., (2012) also found in their evaluation of the KiVa Program that teacher support of the program was positively related to implementation adherence, which in turn contributes to the potential for enhanced program effects. KiVa has only been tested in Europe, although there are currently efforts under way to adapt the model for use in other countries such as the United States.
A recent meta-analysis examining developmental differences in the effectiveness of anti-bullying programs provides some supportive evidence for significant declines in program effectiveness for students in eighth grade and beyond (Yeager et al., 2015). Specifically, Yeager and colleagues examined hierarchical within-study moderation of program effects by age as compared to more typical meta-analytic approaches that examine between-study tests of moderation. Their findings are inconsistent with the findings of Ttofi and Farrington (2009), in which larger program effect sizes (reductions in perpetrating and being a target of bullying) were found for programs implemented with older students (typically defined as students over age 11) compared to younger students.
A number of social-emotional learning programs have also been developed and tested to determine impacts on a range of student outcomes (Durlak et al., 2007, 2011). Some of these models have shown promising effects on aggression and bullying-related outcomes. One such model is Second Step: A Violence Prevention Curriculum. This classroom-based curriculum for children of ages 4-14 aims to reduce impulsive, high-risk, and aggressive behaviors while increasing social-emotional competence and protective factors. The curriculum teaches three core competencies: empathy, impulse control and problem solving, and anger management (Flannery et al., 2005; Baughman Sladky et al., 2015). Students participate in 20-50-minute sessions two to three times per week, in which they practice social skills. Parents can participate in a six-session training that familiarizes them with the content in the children’s curriculum. Teachers also learn how to deal with disruptions and behavior management issues. (Flannery et al., 2005). In one study, children in the Second Step Program showed a greater drop in antisocial behavior compared to those who did not receive the program, behaved less aggressively, and were more likely to prefer prosocial goals
(Flannery et al., 2005; Frey et al., 2005). Other studies of Second Step have demonstrated significant reductions in reactive aggression scores for children in kindergarten through second grade and significant reductions in teacher-rated aggression for the children rated highest on aggression at baseline (Hussey and Flannery, 2007).
In a RCT of 36 middle schools, Espelage et al. (2013) found that students in Second Step intervention schools were 42 percent less likely to self-report physical aggression than students in control schools, with aggression measured as incidents of fighting, but the authors reported that the program had no effect on verbal/relational bullying perpetration, peer victimization,3 homophobic teasing, or sexual violence. In one of the first school-level RCTs of a violence prevention curriculum, Grossman and colleagues (1997) examined, via parent and teacher reports and investigator observation, the effects of the Second Step preventive intervention program on elementary student (second and third grade) aggressive and prosocial behavior. While they did not find changes over time in parent or teacher reports, behavioral observations of students in various school settings showed an overall decrease 2 weeks after the curriculum in physical aggression (–0.46 events per hour, p = .03) and an increase in neutral/prosocial behavior (+3.96 events per hour, p =.04) in the intervention group compared with the control group. One of the recurrent limitations faced by school-level analyses is that measures that have been validated as school-level constructs may not use measures that have only been validated for individual assessment. Similarly, analyses in many studies do not account for the nesting of students within classrooms or schools.
The Good Behavior Game is an elementary school-based prevention program that targets antecedents of youth delinquency and violence. It uses classroom behavior management as a primary strategy to improve on-task behavior and decrease aggressive behavior (Baughman Sladky et al., 2015). Evaluations of the Good Behavior Game in early elementary school have shown it results in reduced disruptive behavior, increased academic engagement time, and statistically significant reductions in the likelihood of highly aggressive children receiving a diagnosis of a conduct disorder by sixth grade, as well as a range of positive academic outcomes (Bradshaw et al., 2009a; Wilcox et al., 2008). The effects were generally strongest among the most aggressive boys, who, when exposed to the program starting in the first grade, had lower rates of antisocial personality disorder when diagnosed as young adults (Petras et al., 2008) and reduced rates of mental health service use, compared to those in the control group (Poduska et al., 2008).
Good Behavior Game has also been tested in combination with other
___________________
3 Peer victimization was assessed using the three-item University of Illinois Victimization Scale (Espelage et al., 2013).
programs, such as Linking the Interests of Families and Teachers (LIFT), which combines school-based skills training with parent training for first and fifth graders. This program is implemented over the course of 21 one-hour sessions delivered across 10 weeks. LIFT uses a playground peer component to encourage positive social behavior and a 6-week group parent-training component. The Good Behavior Game is the classroom-based component of LIFT. LIFT also reduced playground aggression, reduced overall rates of aggression, and increased family problem solving (Eddy et al., 2000; Baughman Sladky et al., 2015).
Raising Healthy Children (Catalano et al., 2003), formerly known as the Seattle Social Development Project (Hawkins et al., 1999), is a multidimensional intervention that targets both universal populations and high-risk youth in elementary and middle school. The program uses teacher and parent training, emphasizing classroom management for teachers and conflict management, problem-solving, and refusal skills for children. Parents receive optional training programs that target rules, communication, and strategies to support their child’s academic success. Follow-up at age 18 showed that the program significantly improved long-term attachment and commitment to school and school achievement and reduced rates of self-reported violent acts and heavy alcohol use (Hawkins et al., 1999). At age 21, students who had received the full intervention when young were also less likely to be involved in crime, to have sold illegal drugs in the past year, or to have received a court charge (Hawkins et al., 2005).
Steps to Respect is another multicomponent program that includes activities led by school counselors for youth involved in bullying, along with schoolwide prevention, parent activities and classroom management. (Frey et al., 2005, 2009; Baughman Sladky et al., 2015). One RCT of Steps to Respect showed a reduction of 31 percent in the likelihood of perpetrating physical bullying in intervention schools relative to control schools (adjusted odds ratio = 0.609) based on teacher reports of student behaviors (Brown et al., 2011). Brown and colleagues (2011) also showed significant improvements in student self-reports of positive school climate, increases in student and teacher/staff bullying prevention and intervention, and increases in positive bystander behavior for students in intervention schools compared to students in control schools (effect sizes ranged from 0.115 for student bullying intervention to 0.187 for student climate). They found no effects for student attitudes about bullying.
In a separate RCT of Steps to Respect, Frey and colleagues (2009) found, using teacher observations of student playground behaviors, statistically significant declines over 18 months in bullying (d = 2.11, p < .01), victimization (d = 1.24, p < .01) and destructive bystander behavior (d = 2.26, p < .01) for students in intervention schools compared to students in con-
trol schools. While student self-reports of victimization declined across 18 months, student self-reports of aggressive behavior did not change.
One of the most comprehensive, long-term school-based programs that has been developed to prevent chronic and severe conduct problems in high-risk children is Fast Track. Fast Track is based on the view that antisocial behavior stems from the interaction of influences across multiple contexts such as school, home, and the individual (Conduct Problems Prevention Research Group, 1999). The main goals of the program are to increase communication and bonds between and among these three domains; to enhance children’s social, cognitive, and problem-solving skills; to improve peer relationships; and ultimately to decrease disruptive behavior at home and in school. Fast Track provides a continuum of developmentally sequenced preventive intervention spanning grades 1 through 10. It includes some of the program elements and frameworks mentioned above, such as a social-emotional learning curriculum developed in elementary school called Promoting Alternative Thinking Strategies, as well as a version of the Coping Power program for higher-risk students. Other elements include support to parents, which is tailored to meet the unique needs of the family and youth.
Thus, Fast Track is a combination of multiple programs across the tiers. It has demonstrated effectiveness in reducing aggression and conduct problems, as well as reducing associations with deviant peers, for students of diverse demographic backgrounds, including sex, ethnicity, social class, and family composition differences (Conduct Problems Prevention Research Group, 2002, 2010; National Center for Health Statistics and National Center for Health Services Research, 2001). In an examination of the longitudinal outcomes of high-risk children who were randomly assigned by matched sets of schools to intervention and control conditions, the Conduct Problems Prevention Research Group (2011) showed that 10 years of exposure to Fast Track intervention prevented lifetime prevalence (assessed in grades 3, 6, 9, and 12) of psychiatric diagnoses for conduct disorder, oppositional defiant disorder, externalizing disorder, and attention deficit hyperactivity disorder.
In addition, a recent RCT of Fast Track showed that early exposure to the intervention substantially reduced adult psychopathology at age 25 among high-risk early-starting conduct-problem children (Dodge et al., 2015). Specifically, intent-to-treat logistic regression analyses showed that 69 percent of participants in the control condition displayed at least one externalizing, internalizing, or substance use psychiatric problem (assessed via self-report or peer interview) at age 25, compared to 59 percent of those assigned to intervention (OR = 0.59, 95% CI [0.43, 0.81]; number needed to treat = 8). Intervention participants also received lower severity-weighted violent crime conviction scores (standardized estimate = −0.37). This study was a random assignment of nearly 10,000 kindergartners in three cohorts,
who were followed through a 10-year intervention and then assessed at age 25 via arrest records, condition-blinded psychiatrically interviewed participants, and interview of a peer knowledgeable about the participant.
The above descriptions of the selected universal multicomponent programs that address bullying or related behavior and their tiered levels of prevention are summarized in Table 5-1. The ecological contexts in which these programs operate are summarized in Table 5-2.
| Program | Origin | Program Type | Typical Delivery Setting |
|---|---|---|---|
| Olweus Bullying Prevention Program | Norway | Bullying prevention, school, school climate, environmental strategies | School |
| Positive Behavioral Interventions and Supports (PBIS) | School climate, academic engagement, behavioral support, interpersonal skills, school/classroom environment | School | |
| KiVa Antibullying Program | Finland | Classroom curricula, school/classroom environment, bullying prevention/intervention, children exposed to violence | School |
| Second Step: A Violence Prevention Curriculum | U.S. | Social-emotional curricula, conflict resolution/interpersonal skills, school/classroom environment, bullying prevention/intervention | School |
Examples of School-Based Selective and Indicated Prevention Programs to Address Bullying or Related Behaviors
As noted above, many of the schoolwide and universal prevention models included elements across the tiers, but here the committee considers programs that are largely focused at the selective and indicated level. Within schools, it is common for students who are involved in bullying to
| Targeted Population | Age Range of Children Served | Program Goals |
|---|---|---|
| Children in kindergarten and elementary, middle, and high schools | 5-18 |
|
| Children in preschool, kindergarten, and elementary, middle, and high schools | 4-18 |
|
| All children | 5-14 |
|
| Children in preschool/kindergarten, elementary school, and middle school | 5-12 |
|
| Program | Origin | Program Type | Typical Delivery Setting |
|---|---|---|---|
| Steps to Respect | U.S. | Bullying prevention, teacher training, social-emotional curricula, conflict resolution/interpersonal skills, school/classroom environment | School |
| Good Behavior Game | U.S. | Classroom management, classroom environment | School |
| Linking the Interests of Families and Teachers (LIFT) | U.S. | Academic engagement, classroom curricula, conflict resolution/interpersonal skills, parent training, school/classroom environment, children exposed to violence, alcohol and drug abuse prevention | School |
| Raising Healthy Children | U.S. | Academic engagement, conflict resolution/interpersonal skills, parent training, school/classroom environment, alcohol and drug abuse prevention | Home, School |
| Fast Track | U.S. | Academic engagement, social-emotional curricula, classroom curricula, conflict resolution/interpersonal skills, parent training, school/classroom environment | School |
SOURCE: Program information was obtained from Blueprints for Healthy Youth Development at http://www.blueprintsprograms.com/programs [June 2016] and CrimeSolutons.gov at http://www.crimesolutions.gov/ [June 2016].
| Targeted Population | Age Range of Children Served | Program Goals |
|---|---|---|
| Students in elementary and middle schools | 8-12 |
|
| Children in kindergarten, elementary school | 6-10 |
|
| Children in elementary school and their families | 6-11 |
|
| Children and their families | 7-16 |
|
| Children identified for disruptive behavior and poor peer relations. | 5-15 |
|
NOTE: The information provided in Table 5-1 is meant to illustrate core features of program elements and focus rather than provide a detailed assessment of all aspects of a program or its demonstrated effects. The table is not intended to be an exhaustive list of all prevention pograms.
| PROGRAM | ||||||
| Olweus Bullying Prevention Program | ||||||
| Positive Behavioral Interventions and Supports | ||||||
| KiVa Antibullying Program | ||||||
| Second Step: A Violence Prevention Curriculum | ||||||
| Steps to Respect | ||||||
| Good Behavior Game | ||||||
| Linking the Interests of Families and Teachers | ||||||
| Raising Healthy Children | ||||||
| Fast Track | ||||||
NOTE: The information provided in Table 5-2 is meant to illustrate core features of program elements and focus rather than provide a detailed assessment of all aspects of a program or its demonstrated effects. The table is not intended to be an exhaustive list of all prevention programs.
SOURCE: Program information was obtained from Blueprints for Healthy Youth Development at http://www.blueprintsprograms.com/programs and CrimeSolutons.gov at http://www.crimesolutions.gov/ [June 2016].
be referred for some type of school-based or community counseling services (Swearer et al., 2014).
McElearney and colleagues (2013) reported that school counseling was an effective intervention for middle school students who had been bullied when the counseling focused on improving peer relationships. In their study, they collected longitudinal data from 202 students (mean age = 12.5) using
the self-rated Strengths and Difficulties Questionnaire (SDQ).4 In total, 27.2 percent of the student referrals to the intervention related to being bullied. Students who had been bullied had significantly higher initial status scores (LGC initial score = 1.40, p < .001) on the Peer Problems subscale of the SDQ and experienced a significantly more rapid rate of decrease on this subscale (LGC rate of change score = −0.25, p < .001) with each successive session of school counseling, compared with those students who had accessed the intervention for another reason. However, counseling sessions probably vary considerably in the services provided and the extent to which they employ evidence-based models.
A few studies have examined social workers or school mental health staff who provide intervention for youth involved in bullying, but the research in this area is rather weak, with relatively few systematic studies focused on assessing the impacts of selective and indicated programs on bullying (Swearer et al., 2014). Moreover, given the difficulty of determining the efficacy of counseling as an intervention per se, the committee focuses here more specifically on particular structured preventive intervention models that have been more formally articulated in a curriculum, many of which are delivered by school-based counselors, social workers, or psychologists.
For example, Berry and Hunt (2009) found preliminary support for a cognitive-behavioral intervention for anxious adolescent boys in grades 7-10 (mean age of 13.04 years) who had experienced bullying at school. Fung (2012) assessed a group treatment for youth ages 11-16, provided by social workers in Hong Kong using a social information processing model. Students were selected for intervention based on their high levels of aggressive behavior rather than bullying specifically, but the author did find that after 2 years of the intervention, students reported a decrease in reactive aggression but not proactive aggression. Fung (2012) also found that cognitive-behavioral group therapy was effective in reducing anxious and depressed emotions in children who are both the perperator and target of bullying.
One of the few evidence-based targeted intervention programs for late preadolescent children is the Coping Power Program (Lochman et al., 2013). Coping Power targets aggressive youth and their parents and is delivered by counselors in small groups over the course of a school year. Additional supports are provided to teachers to promote generalization of skills into nongroup settings. The program has demonstrated significant improvements in aggressive-disruptive behaviors and social interactions, many of which were maintained at 3-year follow-up for children from fourth through sixth grade (Lochman et al., 2013).
___________________
4 The SDQ is a brief behavioral screening questionnaire that asks about 25 attributes, some positive and others negative (Goodman, 1997).
Having available strategies to cope with stress has also been shown to reduce depression among older adolescents who were bullied (Hemphill et al., 2014). Although originally developed for students in grades 4-6, there is currently an ongoing 40-school randomized trial testing a middle school version of this model; the trial has a particular focus on assessing outcomes related to bullying (Bradshaw et al., in press); a high school model of Coping Power is also currently in development and will soon be tested on 600 urban high school students (Bradshaw et al., in press).
DeRosier (2004) and DeRosier and Marcus (2005) evaluated the effects of a social-skills group intervention for children experiencing peer dislike, bullying, or social anxiety. In their study of third graders randomly assigned to treatment or to no-treatment control, DeRosier and Marcus (2005) showed that aggressive children exposed to the program reported greater declines in aggression and bullying behavior and fewer antisocial affiliations than aggressive children in the no-intervention control condition. The intervention resulted in decreased aggression on peer reports (Cohen’s d = 0.26), decreased targets of bullying on self-reports (Cohen’s d = 0.10) and fewer antisocial affiliations on self-reports (Cohen’s d = 0.11) for the previously aggressive children (DeRosier and Marcus, 2005).
A study of elementary school students exposed to the FearNot! virtual learning intervention to enhance coping skills of children who were bullied showed a short-term improvement on escaping being bullied (Sapouna et al., 2010). In a separate evaluation of the FearNot! Program in the UK and German schools, exposure to the intervention was found to help non-involved primary grade children to become defenders of the target in virtual bullying situations, at least for youth in the German sample (Vannini et al., 2011).
There are also a number of preventive interventions that aim to address mental health problems but may also prove to be helpful for youth who are involved in bullying. For example, a school-based version of cognitive-behavioral therapy is Cognitive Behavioral Intervention for Trauma in Schools (CBITS). This evidence-based treatment program is for youth ages 10-15 who have had substantial exposure to violence or other traumatic events and who have symptoms of posttraumatic stress disorder (PTSD) in the clinical range. The CBITS Program has three main goals: (1) to reduce symptoms related to trauma, (2) to build resilience, and (3) to increase peer and parent support. Based on a model of trauma-informed care, CBITS was developed to reduce symptoms of distress and build skills to improve children’s abilities to handle stress and trauma in the future. The intervention incorporates cognitive-behavioral therapy skills in a small group format to address symptoms of PTSD, anxiety, and depression related to exposure to violence. CBITS was found to be more accessible to families who may not have been able or willing to participate outside of schools. CBITS was also
found to significantly improve depressive symptoms in students with PTSD (Jaycox et al., 2010).
Examples of Family-Focused Preventive Interventions to Address Bullying
A few family-focused preventive interventions have been developed that may also demonstrate promising effects on bullying. For example, the Incredible Years Program aims to reduce aggressive and problem behaviors in children, largely through supports to parents, as well as students and teachers. It focuses on social skills training components (Webster-Stratton, 1999) and targets elementary school students with the aim of preventing further aggression and related behavior problems for youth with conduct problems but whose behavior would not yet be considered in the clinical range requiring treatment. Barrera and colleagues (2002) showed that high-risk elementary school children in the Incredible Years Program displayed lower levels of negative social behavior, including aggression, compared to control youth who did not receive the intervention. In another study, Webster-Stratton and colleagues (2008) showed that teacher training in combination with Dinosaur School in Head Start and first grade classrooms with at-risk students resulted in improved social competence and self-regulation and in fewer youth conduct problems. There is also a universal version of the Incredible Years Program delivered by teachers, which is currently being tested in two separate randomized trials. To the committee’s knowledge, bullying has not been assessed as an outcome in prior studies of Incredible Years, although several impacts on other discipline and behavior problems have been observed in prior RCTs.
Another family-focused program is The Family Check-Up (also known as the Adolescent Transitions Program). This multilevel, family-centered intervention targets children at risk for problem behaviors or substance use. The Family Check-Up had historically been delivered in middle school settings, but more recent studies have extended the model to younger populations (e.g., 2-5 year olds in Dishion et al., 2014). Parent-focused elements of The Family Check-Up concentrate on developing family management skills such as using rewards, monitoring, making rules, providing reasonable consequences for rule violations, problem solving, and active listening (Dishion and Kavanagh, 2003). Connell and colleagues (2007) found that The Family Check-Up resulted in significantly fewer arrests; less use of tobacco, alcohol, and marijuana; and less antisocial behavior for intervention youth, compared with control group youth.
Another targeted program that includes supports for families is the Triple P intervention. A RCT of Resilience Triple P for Australian youth 6 to 12 years old found significant improvements for intervention youth compared to controls on teacher reports of overt victimization (d = 0.56),
and child overt aggression toward peers (d = 0.51) as well as improvements in related mental health such as internalized feelings and depressive symptoms. The intervention that combined facilitative parenting with social and emotional skills training worked best (Healy and Sanders, 2014). An earlier study of Triple P for preschoolers at risk for conduct problems found that a version delivered by practitioners (clinical psychologists, psychologists, and psychiatrists) trained and supervised in the delivery of the interventions was more effective in reducing problem behaviors compared to a wait-list condition and a Triple P program that was self-directed (Sanders et al., 2000).
In addition to the largely school- and family-based programs summarized above, there are several evidence-based interventions that are more typically provided in the community (Baughman Sladky et al., 2015). Although these programs focus more generally on violence and aggression prevention, they may also produce effects on bullying related behaviors, such as conduct problems for perpetrators or those at risk for perpetration, or they may address the behavioral and mental health consequences of being bullied.
For example, a widely utilized intervention to address mental health issues for children and adolescents is Trauma Focused Cognitive Behavioral Therapy (TF-CBT) which has been shown to be effective in reducing mental health symptoms related to violence exposure (Cohen et al., 2006). TF-CBT has been particularly effective in treating children who are victims of sexual abuse (Cohen et al., 2005). While not specifically used to address being a target of bullying, TF-CBT can be used to treat complex trauma and has been shown to result in improvements to mental health issues related to peer victimization including PTSD symptoms, depression, anxiety, and externalizing behavior problems (Cohen et al., 2004; Deblinger et al., 2011).
Programs that are delivered in the community often include supports for parents as well as the youth. For example, Functional Family Therapy (FFT) is a family-based intervention program that targets youth between the ages of 11 and 18 who are at risk for and/or presenting with delinquency, violent or disruptive behavior, or substance use (Baughman Sladky et al., 2015). It is time-limited, averaging 8-12 sessions for referred youth and their families, with generally no more than 30 hours of direct service time for more difficult cases. FFT is multisystemic and multilevel in nature, addressing individual, family, and treatment system dynamics. It integrates behavioral (e.g., communication training) and cognitive-behavioral interventions (e.g., a relational focus). Assessment is an ongoing and multifaceted part of each phase (Henggeler and Sheidow, 2012). Evaluations of FFT have shown significant improvements in delinquent behavior and recidivism (Aos et al., 2011; Sexton and Alexander, 2000).
Brief Strategic Family Therapy (BSFT) is a short-term (approximately 12-15 sessions over 3 months) family-based intervention for children and youth ages 6-17 who are at risk for substance abuse and behavior prob-
lems (Robbins et al., 2002, 2007; Szapocznik and Williams, 2000). BSFT employs a structural family framework and focuses on improving family interactions. Evaluation results demonstrate decreases in substance abuse, conduct problems, associating with antisocial peers, and improvements in family functioning. In a small randomized trial of girls who were perpetrators of bullying, Nickel and colleagues (2006) found a decrease in bullying behavior (and expressive aggression) in the BSFT group, with improvements maintained at 1-year follow-up. Similar findings were observed in a separate study of BSFT for boys who were involved in bullying behavior. (Nickel et al., 2006).
Wraparound/Case Management is a multifaceted intervention designed to keep delinquent youth at home and out of institutions by “wrapping” a comprehensive array of individualized services and support networks “around” young people, rather than forcing them to enroll in predetermined, inflexible treatment programs (Bruns et al., 1995; Miles et al., 2006). Evaluations of Wraparound have found marked improvement in behavior and socialization, and youth in the intervention group were significantly less likely to reoffend compared to graduates of conventional programs (Carney and Buttell, 2003; Miles et al., 2006).
Multisystemic Therapy (MST) targets chronic, violent, or substance-abusing male or female juvenile offenders, ages 12-17, at risk of out-of-home placement, along with their families. MST is a family-based model that addresses multiple factors related to delinquency across key socioecological settings. It promotes behavior change in the youth’s natural environment, using a strengths-based approach (Henggeler, 2011). Critical service characteristics include low caseloads (5:1 family-to-clinician ratio), intensive and comprehensive services (2-15 hours per week) and time-limited treatment duration (4-6 months) (Henggeler et al., 1999). Treatment adherence and fidelity are key ingredients for achieving long-term, sustained effects and decreasing drug use. Evaluations of MST that examined delinquency rates for serious juvenile offenders demonstrated a reduction in long-term rates of re-arrest, reductions in out-of home placements, and improvements in family functioning, and decreased mental health problems for serious juvenile offenders (Greenwood and Welsh, 2012; Schaeffer and Borduin, 2005). A recent meta-analysis of the effectiveness of MST across 22 studies containing 322 effect sizes found small but statistically significant treatment effects for its primary outcome of delinquent behavior, but the meta-analysis also found secondary outcomes such as psychopathology, substance use, family factors, out-of-home placements, and peer factors. For example, considering MST as an intervention that may affect bullying related behaviors, eight studies assessing peer relations showed improvements for aggressive youth treated with MST compared to youth treated via other modalities (mean effect size d = 0.213) (van der Stouwe et al., 2014).
Another communitywide prevention model that holds promise for reducing violence and related behavior problems is the Communities That Care (CTC) framework. CTC is a system for planning and organizing community resources to address adolescent problematic behavior such as aggression or drug use. It has five phases to help communities work toward their goals. The CTC system includes training events and guides for community leaders and organizations. The main goal is to create a “community prevention board” comprising public officials and community leaders to identify and reduce risk factors while promoting protective factors by selecting and implementing tested interventions throughout the community. Based on communitywide data on risk and protective factors, schools may select from a menu of evidence-based programs, which includes some of
| Program | Origin | Program Type | Typical Delivery Setting |
|---|---|---|---|
| Coping Power Program | U.S. | Cognitive behavioral treatment, parent training, social-emotional learning | School |
| Incredible Years | U.S. | Academic engagement, cognitive behavioral treatment, social-emotional curricula, conflict resolution/interpersonal skills, family therapy, group therapy, parent training, school/classroom environment | Home, school, community |
| The Family Check-Up (formerly Adolescent Transitions) | U.S. | Academic engagement, crisis intervention/response, family therapy, parent training, school/classroom environment, motivational interviewing | School |
| Triple P | Australia | Parent training | School, community, home, hospital/medical center, mental health/treatment center |
the models listed above. Thus, CTC is more of a data-informed process for selecting and implementing multiple evidence-based programs. As a result, it is difficult to attribute significant improvements in youth behavior to any one specific program. However, randomized studies testing the CTC model have shown statistically significant positive effects on delinquency, alcohol use, and cigarette use, all of which were lower by grade 10 among students in CTC communities, compared to students in control communities (Hawkins et al., 2011).
Descriptions of a subset of selective and indicated prevention programs that address bullying or related behavior and their tiered level of prevention are summarized in Table 5-3. The ecological contexts in which these programs operate are summarized in Table 5-4.
| Targeted Population | Age Range of Children Served | Program Goals |
|---|---|---|
| Aggressive youth and their parents | 8-15 |
|
| Children at high risk for problem behaviors or substance use, along with their parents and teachers | 2-8 |
|
| Families | 2-7 |
|
| Parents with a child in the age range between birth and 12 years | 0-12 |
|
| Program | Origin | Program Type | Typical Delivery Setting |
|---|---|---|---|
| Cognitive Behavioral Intervention for Trauma in Schools (CBITS) | Cognitive behavioral treatment, group therapy, individual therapy, school/classroom environment, trauma-informed | School, high crime neighborhood/hot spots | |
| Trauma Focused Cognitive Behavioral Therapy (TF-CBT) | Cognitive behavioral treatment, family therapy, parent training, trauma-informed | Inpatient/out-patient | |
| Functional Family Therapy (FFT) | U.S. | Family therapy, individual therapy, probation/parole services | Inpatient/outpatient, home, community |
| Brief Strategic Family Therapy (BSFT) | U.S. | Alcohol and drug therapy/treatment, conflict resolution/interpersonal skills, family therapy, parent training, alcohol and drug prevention | Home, workplace, community |
| Wraparound/Case Management | U.S. | Individualized case management via team planning that is family-driven, culturally competent, and community-based | Home, community |
| Multisystemic Therapy (MST) | U.S. | Alternatives to detention, cognitive behavioral treatment, conflict resolution/interpersonal skills, family therapy, individual therapy, parent training | Home, community, school |
| Communities That Care (CTC) | U.S. | Classroom curricula, school/classroom environment, community crime prevention, alcohol and drug prevention | School, community |
NOTE: The information provided in Table 5-3 is meant to illustrate core features of program elements and focus rather than provide a detailed assessment of all aspects of a program or its demonstrated effects. The table is not intended to be an exhaustive list of all prevention programs.
| Targeted Population | Age Range of Children Served | Program Goals |
|---|---|---|
| Children exposed to violence or other traumatic events |
|
|
| Children exposed to violence and their families | 3-14 |
|
| Young offenders and their families | 11-18 |
|
| Children at risk for substance abuse and behavior problems and their families | 6-17 |
|
| Children and their families | 6-18 |
|
| Young offenders and their families | 12-17 |
|
| Infant, early childhood-preschool, late childhood, kindergarten-elementary school, early adolescence, middle school, late adolescence, high school, early adulthood | 0-18 |
|
SOURCE: Program information was obtained from Blueprints for Healthy Youth Development at http://www.blueprintsprograms.com/programs and CrimeSolutons.gov at http://www.crimesolutions.gov/ [June 2016].

NOTE: The information provided in Table 5-4 is meant to illustrate core features of program elements and focus rather than provide a detailed assessment of all aspects of a program or its demonstrated effects. The table is not intended to be an exhaustive list of all prevention programs.
SOURCE: Program information was obtained from Blueprints for Healthy Youth Development at http://www.blueprintsprograms.com/programs [June 2016] and CrimeSolutons.gov at http://www.crimesolutions.gov/ [June 2016].
Examples of Preventive Intervention to Address Cyberbullying and Related Behaviors
In a review of interventions to reduce cyberbullying, Mishna and colleagues (2012) found some gains in knowledge about Internet safety, but psychoeducational interventions had little effect on changing risky online behavior. Ryan and Curwen (2013) noted the lack of evidence-based interventions for victims of cyberbullying in their review of evidence regarding the occurrence, impact, and interventions for targets of cyberbullying. Given that cyberbullying takes place online and that the vast majority of youth are online, online resources to prevent or address cyberbullying may have broad reach. At present, online resources exist that were created to address or provide support regarding cyberbullying; one example is the website STOP Cyberbullying.5 There have also been social marketing campaigns tied to online resources that include resources to counter cyberbulling; one example is the It Gets Better Project.6 To the committee’s knowledge, none of these online programs has undergone empirical evaluation yet.
Across social media sites, there is no consistent information about bullying policies, resources, or tracking of behaviors. Facebook is the most popular social media site and provides a Webpage of bullying resources.7 Instagram is also popular among teens and provides its own Webpage discussing cyberbullying.8 Both of these sites provide links where bullying can be reported to site administrators, but there are no published reports of this information or empirical studies evaluating prevalence of what is reported. The committee found no studies of the effectiveness of these sites or of the resources they provide.
In the family context, however, recent correlational studies suggest that spending time together, such as through family meals, may provide an important context for disclosure of being a target of bullying, which in turn buffers some of the subsequent effects of bullying on social-emotional adjustment (Elgar et al., 2014).
Some recent research, predominantly in Europe, has examined the effectiveness of preventive interventions specifically on cyberbullying. These programs are school based and were designed for students between the ages of 13 and 17. Many of these evaluation studies used randomized designs, including studies of Cyber Friendly Schools and the Viennese Social Competence Program. Cyber Friendly Schools is a whole-school, online cyberbullying prevention and intervention program that is based on a
___________________
5 See http://www.stopcyberbullying.org [April 2016].
6 See http://www.itgetsbetter.org/ [April 2016].
7 See Put a Stop to Bullying at https://www.facebook.com/safety/bullying [February 2016].
8 See Learn How to Address Abuse at https://help.instagram.com/527320407282978/ [October 2015].
social–ecological approach and considers the many factors that influence students’ vulnerability to cyberbullying at multiple levels (Cross et al., 2015). The Viennese Social Competence Program is a primary preventive program that includes secondary preventive elements to reduce aggressive behavior and bullying and to foster social and intercultural competencies in schools (Gradinger et al., 2015). These programs have been associated with declines, from program pretest to post-test, in both cyberbullying perpetration and being targeted.
The German program Medienhelden (“Media Heroes”), which was originally designed for traditional bullying, has also been used as a cyberbullying intervention. This program is a universal, modularized, and theoretically based preventive intervention for the school context that builds on previous knowledge about potential risk and protective factors such as cognitive and affective empathy. An evaluation of this program showed that while the intervention was associated with reductions in both traditional and cyberbullying perpetration for both short-intervention conditions (mean difference = −0.29, p = .00) and long-intervention conditions (mean difference = −0.32, p = .00), it was not associated with reductions in being targets of either kind of bullying (Chaux et al., 2016).
Other studies used a quasi-experimental design. For example, an evaluation of the NoTrap! Program, which is a school-based intervention, and utilizes a peer-led approach to prevent and combat both traditional bullying and cyberbullying, showed a decrease over time in being targeted for traditional bullying or cyberbullying (F(1, 457) = 5.379, p = .02; η2p = .012) and in perpetrating bullying (F(1, 457) = 9.807, p =. 002; η2p = .021) (Palladino et al., 2016). Evaluation of the ConRed Program (Ortega-Ruiz et al., 2012), which is a theory-driven program designed to prevent cyberbullying and improve cyberbullying coping skills, showed that individuals who had been targets of cyberbullying reported decreased incidence of being bullied for both traditional bullying (F = 7.33, p = .008, d = 0.46) and cyberbullying (F = 7.73, p = .03, d = 0.56) (Del Rey et al., 2015). Finally, a study focused on college students used the theory of reasoned action (Ajzen, 1985) in a cyberbullying prevention program involving an educational video. One month follow-up found that the intervention group had increases in cyberbullying knowledge (d = 0.85), as well as decreases in approving attitudes (.24 < ds < .48) toward online behaviors such as unwanted contact, public humiliation, and deception (Doane et al., 2015).
As a whole, this body of research supports a finding that interventions designed to target one type of bullying can have spillover effects on another. This is not surprising, given the overlap between cyberbullying and traditional bullying (Waasdorp and Bradshaw, 2015). A common issue and limitation of this body of work is that all the studies involved self-report by students. Future research opportunities include triangulating this data
with reports from parents or teachers. All of the preventive interventions reviewed in this section, despite their focus on cyberbullying, are implemented in the offline world and specifically in schools.
RECOMMENDED COMPONENTS AND CONSIDERATIONS FOR BULLYING PREVENTION
In the committee’s broader reflections on the literature about and practice of bullying prevention, a number of core elements or critical features consistently emerged. In this section, we summarize those elements for which there is a converging body of supporting evidence. However, a challenge in this area is the limited documentation on the effectiveness of particular components or programmatic elements. Much of what has been reported about what works in bullying prevention comes from randomized trials of programs and meta-analyses summarizing effective models, with limited post hoc exploration into programmatic elements associated with the greatest effect sizes. Although few studies were appropriately designed to discern particular effective components or elements of an entire model, separate from other elements, the following frameworks and core components are among the most promising within the extant research.
As noted above, there is a growing emphasis on the use of multi-tiered approaches—those which leverage universal, selective, and indicated prevention programs and activities. For example, a tiered approach might include lessons on social-emotional skill development for all students—thus making it a universal program. In fact, research highlights the importance of providing class time to discuss bullying (Olweus, 1993) and the use of lessons to foster skills and competencies, effective communication, and strategies for responding to bullying (Farrington and Ttofi, 2009); such strategies can also have a positive impact on academic and other behavioral outcomes (Durlak et al., 2010). Effective classroom management is also critical, as well-managed classrooms are rated as having a more favorable climate, being safer and more supportive, and having lower rates of bullying compared to less-well-managed classrooms (Koth et al., 2008). At Tier 2, selective interventions may include social skills training for small groups of children at risk for becoming involved in bullying. Finally, an indicated preventive intervention (Tier 3) may include more intensive supports and programs tailored to meet the needs of students identified as a perpetrator or a target of bullying and the needs of their families (Espelage and Swearer, 2008; Ross and Horner, 2009).
Consistent with the social–ecological framework (Espelage et al., 2004), schools should address the social environment and the broader culture and climate of bullying (Bradshaw and Waasdorp, 2009). Research documents the importance of schoolwide prevention efforts that provide
positive behavior support, establish a common set of expectations for positive behavior across all school contexts, and involve all school staff in prevention activities (Ross and Horner, 2009). Effective supervision, especially in bullying “hot spots,” and clear anti-bullying policies are essential elements of a successful schoolwide prevention effort (Olweus, 1993). The playground appears to be a particularly important context for increasing supervision in order to prevent bullying (Farrington and Ttofi, 2009; Frey et al., 2005). Collecting data on bullying via anonymous student surveys can inform the supervision and intervention process. These data can identify potential areas for intensive training of school staff, which is an essential element of successful bullying prevention efforts (Farrington and Ttofi, 2009). Data are also critical for monitoring progress toward the goal of reducing bullying (Olweus, 1993).
Families also play a critical role in bullying prevention by providing emotional support to promote disclosure of bullying incidents and by fostering coping skills in their children. Parents need training in how to talk with their children about bullying (Johnson et al., 2011), how to communicate their concerns about bullying to the school, and how to get actively involved in school-based bullying prevention efforts (Waasdorp et al., 2011). There also are important bullying prevention activities that can occur at the community level, such as awareness or social marketing campaigns that encourage all youth and adults—including doctors, police officers, and storekeepers—to intervene when they see bullying and to become actively involved in school- and community-based prevention activities (Olweus, 1993).
It is also important to consider how schools can integrate prevention efforts with their other existing programs and supports. Research by Gottfredson and Gottfredson (2001) indicates that, on average, schools are using about 14 different strategies or programs to prevent violence and promote a safe learning environment. This can often be overwhelming for school staff to execute well, thereby leading to poor implementation fidelity. Therefore, schools are encouraged to integrate their prevention efforts so that there is a seamless system of support (Domitrovich et al., 2010), which is coordinated, monitored for high fidelity implementation, and includes all staff across all school contexts. Instead of adopting a different program to combat each new problem that emerges, schools can develop a consistent and long-term prevention plan that addresses multiple student concerns through a set of well-integrated programs and services. Such efforts would address multiple competencies and skills in order to prevent bullying, while helping students cope and respond appropriately when bullying does occur. Programs should include efforts to enhance resilience and positive behaviors and not just focus on reductions in bullying perpetration. The three-tiered public health model provides a framework for connecting bullying
prevention with other programs to address bullying within the broader set of behavioral and academic concerns.
Collectively, the extant research suggests that there are a number of universal prevention programs that are effective or potentially promising for reducing bullying and related behavioral and mental health concerns. With regard to selective and indicated prevention programs, the focus of the model tends to be more generally on other behavioral concerns, with relatively few programs at these levels being tested using RCT designs to determine impacts on bullying specifically. Additional research is clearly needed to better understand the impacts of programs across all three tiers, as well as the combined impacts of such programs.
NONRECOMMENDED APPROACHES
There has been an emerging concern that some programs and strategies commonly used with the goal of preventing or stopping bullying may actually increase bullying or cause other harm to youth or the school community. For example, suspension and related exclusionary techniques are often the default response by school staff and administrators in bullying situations; however, these approaches do not appear to be effective and may actually result in increased academic and behavioral problems for youth. Encouraging youth to fight back when bullied is also not a recommended strategy, as it suggests that aggression is an effective means for responding to victimization and may perpetuate the cycle of violence. Furthermore, such an aggressive response may escalate the level of violence and the risk of harm for all parties involved. While there is still much to be learned about effective youth responses to bullying across the different age groups and social–ecological contexts, recommended responses may include deflecting, seeking peer and adult support, and avoidance of situations that may increase the likelihood of exposure to bullying (Waasdorp and Bradshaw, 2011). Yet there are characteristics of some youth that may make some of these responses easier to display than others. For example, youth who have challenges regulating emotions and inhibiting aggressive responses are more likely to use violence when bullied.
Given that bullying is a complex peer behavior, it may seem wise to leverage peers in attempting to intervene in bullying situations. In fact, there is a large and growing literature supporting the potential effectiveness of bystander interventions (Polanin et al., 2012). However, caution should be taken about the types of roles youth play in bullying prevention. Youth- or peer-facilitated programs, such as peer mediation, peer-led conflict resolution, forced apology, and peer mentoring may not be appropriate or effective in bullying prevention.
There are concerns about approaches based on forced apology or the
use of peer-mediated conflict resolution within the context of bullying programs, in part because of the face-to-face interactions between the youth who have been perpetrators and those who have been targeted. Such approaches are rarely structured in a way to address peer abuse of power, as it occurs in bullying behavior, as compared to the original focus of such approaches on conflict (Bradshaw, 2013). The systematic review and meta-analysis of school-based anti-bullying programs by Ttofi and Farrington (2011) found that programs that were peer-led often produced null or even iatrogenic effects. Some programs appeared to increase attitudes supportive of bullying, whereas others showed an increase in incidents of targeting rather than a reduction in bullying-related behaviors. There is also a large body of violence- and delinquency-related research (see Dodge et al., 2006, for review) suggesting that grouping youth who bully together may actually reinforce their aggressive behaviors and result in higher rates of bullying. In these situations, a contagion process likely occurs, whereby the youth learn more aggressive and bullying behaviors from each other and are reinforced for their aggressive behavior. Furthermore, conflict resolution approaches, even when facilitated by adults, are not typically recommended in situations of bullying, as they suggest a disagreement between two peers of equal status or power, rather than an instance of peer abuse. These approaches also typically bring targets and youth who bully face to face, which may be especially hurtful for the youth who is bullied. It is important to note, however, that there may be other forms of delinquent and problem behavior, such as property offenses or threats toward staff, which may be more appropriate for these types of conflict resolution approaches. Although additional research is certainly needed to determine the appropriateness of these and other youth-facilitated practices in the context of bullying prevention, it is likely that structured and well-supervised youth leadership activities can have a positive impact on bullying prevention; however, more RCT-designed studies that document outcomes associated with these approaches are needed.
There is also little evidence that one-day awareness raising events or brief assemblies are effective at changing a climate of bullying or producing sustainable effects on bullying behavior (Farrington and Ttofi, 2009). Some of these types of efforts have focused largely on instances of youth suicides, which may have been linked in some way with bullying. Given growing concerns about the potential association between bullying and youth suicide, and more generally issues related to suicidal contagion among adolescents (Duong and Bradshaw, 2015; Romer et al., 2006), practitioners and researchers should be cautious in highlighting such a potential link, as it may result in confusion and misattribution among families as well as in the media. Rather, it is critical to state the epidemiologic evidence that suicide is extremely complex and generally associated more directly with
mental health concerns such as anxiety and depression. Bullying could, therefore, serve as a risk factor for youth who are also experiencing mental health concerns (Klomek et al., 2011). This underscores the importance of multicomponent programs that address social, behavioral, and mental health concerns.
AREAS FOR FUTURE RESEARCH RELATED TO BULLYING PREVENTION PROGRAMMING
This final major section of the chapter identifies a number of areas that require additional research and focus in order to advance bullying prevention programming.
Implementation of Bullying Prevention Programming
There is a need for more implementation-focused research aimed at improving the adoption and implementation of evidence-based programs. Numerous studies have documented challenges with implementation fidelity of school-based programs, most of which suggest that the programs themselves are not difficult to implement; rather, constraints such as lack of buy-in, limited time to implement programs, competing priorities, lack of organizational capacity to coordinate the effort, and insufficient administrative support are all factors that may contribute to the relatively slow adoption of school-based programs and that compromise implementation fidelity (Beets et al., 2008; Domitrovich et al., 2008; Vreeman and Carroll, 2007). Commitment not only to the implementation of a model but also to its sustainment and authentic integration with other efforts is needed for any such program to become routinized. For example, teacher attitudes about the potential effectiveness of the program, as well as school-related factors that support successful implementation with fidelity, have been shown to be important predictors of successful implementation of universal character education programs (Beets et al., 2008).
A need also exists for sustained investment in data systems to guide the identification of strengths and gaps in implementation programming, as well as to track progress toward outcomes (Bradshaw, 2013). Adequate time for ongoing quality professional development, coaching supports, and performance feedback are essential features of an implementation support system for achieving high-quality implementation of any evidence-based practice; positive effects cannot otherwise be expected (Domitrovich et al., 2008; Fixsen et al., 2005).
Bullying prevention programming could also benefit from adopting practices and principles from the field of implementation science (Fixsen et al., 2005). It may be that potentially effective programs already exist
and that the field just needs to make a more sustained commitment to implementing the existing models with fidelity and testing them with RCT designs to better understand what works for whom, and under what conditions. This may be especially relevant when considering the broader set of youth violence prevention programs, which have rarely been evaluated to determine the impacts of these interventions on bullying specifically. The field of bullying prevention could benefit from the development and implementation of additional innovative and novel approaches that use emerging technologies and strategies. Furthermore, more research is needed to better understand the effective mechanisms of change and strategies to optimize the effect size of prevention programs.
The Role of Peers and Peer-Led Programming
There is no question that peers have a significant influence on youth development (Collins et al., 2000; Dodge et al., 2006) including their involvement in and responses to bullying (Paluck et al., 2016; Salmivalli, 2010). In fact, correlational studies have found that having more friends was associated with increased bullying perpetration but less risk of being bullied (Wang et al., 2009), whereas other studies found that the way in which peers respond to witnessing bullying may help buffer the effects for the targeted youth (Salmivalli et al., 1996). As a result, there is an increasing interest in leveraging these relationships and influences to prevent and intervene in bullying situations (Paluck et al., 2016). However, the empirical findings on the role of peers in bullying prevention have been mixed, with some researchers suggesting the need for more peer-based interventions (Paluck et al., 2016), such as friendship-making components (Leff and Waasdorp, 2013), and others calling for more caution, particularly regarding implementation of selected or indicated interventions (Dodge et al., 2006). Clearly, there is a need to distinguish between the role of peers as bystanders in bullying situations and peers as potential leaders or implementers of intervention programs.
Within group-based interventions, which is often a modality used for selective and some indicated preventive interventions, studies show that there is the potential for deviance training and a shift in attitudes that actually favor aggression and deviant behavior (Dodge et al., 2006). While there are certainly structures and procedures that adult facilitators of such groups can put in place to try to mitigate these potentially iatrogenic effects, caution should be taken when implementing group-based programs for youth who are aggressive, such as those who bully.
One particular area of interest is intervention programs that operate through peer bystander behavior. This is a topic that is gaining attention, both within practice and within the research literature (Cunningham et
al., 2011; Polanin et al., 2012; Salmivalli, 2014). A bystander is defined as an onlooker who is present during the bullying event but remains neutral (passive), helping neither the victim nor the bully (Salmivalli, 2010). A meta-analysis by Polanin and colleagues (2012) reviewed 12 school-based bullying prevention approaches that focused on bystanders’ behaviors as a component of the intervention. They found that bystander-involved models were generally effective at reducing bullying (overall effect size as measured by Hedge’s g = 0.20, p < .001, 95% CI [0.11, 0.29]). Although overall these programs were successful at increasing bystanders’ intervention in bullying situations, Polanin and colleagues (2012) did not find any improvement in bystander empathy for the victims. This is consistent with other recent meta-analyses on a smaller set of studies that included bystander effects (Merrell et al., 2008). Developmentally, Polanin and colleagues (2012) also found that bystander intervention effects were larger for older youth compared to younger children. Specifically, the effects were typically stronger in high schools (ES = 0.43) compared to students in younger grades (ES = 0.14; p < .05). Polanin and colleagues (2012) noted that their meta-analysis was limited to a relatively small number of studies, so they called for more research on the effects of peers on bullying, especially regarding the distinction between peers as bystanders and peers as leaders of intervention programming.
There are some potentially promising findings emerging from a few peer-led educational models that have been used successfully to address bullying and cyberbullying in Italy (Menesini et al., 2012). Other youth-led programs have demonstrated some potentially promising effects in the context of bullying, sexual harassment, and dating violence prevention (Connolly et al., 2015). However, a study by Salmivalli (2001) testing a peer-led intervention campaign against school bullying found that it produced mixed effects, with an increase in pro-bullying attitudes among boys. Additional research is clearly needed with larger samples and more RCT designs to determine the extent to which these and the other peer-led models are truly effective and robust against potentially iatrogenic effects. Other potentially promising findings are in the area of gay-straight alliances, which were discussed in Chapter 3 (Poteat et al., 2013, 2015). Such resources appear to be an important buffer for LGB youth and may contribute to a shift in the norms regarding stereotype-driven targeting of LGB youth. There is also growing interest in programming focused on issues related to equity in relation to both sexual and racial minorities (Bulanda et al., 2014; Polanin and Vera, 2013). Similarly, there is increasing interest in the use of restorative practice-based models with the goal of preventing bullying and providing more equitable disciplinary practices in response to other behavioral violations (Bradshaw, 2013). However, much of the work on this topic has been descriptive and conceptual, with few randomized
and controlled studies assessing behavioral or bullying-related outcomes for youth. Additional research is needed to leverage findings from the extant research on equity and inclusion for subpopulations (e.g., minorities; youth with disabilities; lesbian, gay, bisexual, and transgender [LGBT] youth) to inform bullying prevention programming.
Role of Educators and School-Based Programming
Given the amount of time youth spend in school and the overall rates of school-based bullying, it is not surprising that teachers and other education support professionals play an important role in bullying prevention (Bradshaw et al., 2013b). Teachers often serve as implementers of programs as well as frontline interveners in bullying situations (Goncy et al., 2014; Holt et al., 2013); however, they vary in their willingness to intervene and in their skills to intervene effectively (Biggs et al., 2008; Bradshaw et al., 2009c; Hektner and Swenson, 2011). In fact, there appears to be a disconnect between students’ and educators’ perceptions and experiences of bullying behavior. Several studies found that educators underestimated the impact and prevalence of bullying behavior (Bradshaw et al., 2009c), which in turn likely contributes to youth’s hesitance to report bullying to adults at school. Furthermore, many adults lacked skills to intervene effectively, and potentially even overestimated their efficacy and ability to detect bullying-related problems. Studies have found that many youth perceived teachers as not effective in preventing or intervening in bullying situations (Berguno et al., 2004; Bradshaw et al., 2009c).
In contrast, teachers’ perceived efficacy has been associated with an increased likelihood of intervening in a bullying situation, although this was also affected by perceived threat and the teachers’ years of experience (Duong and Bradshaw, 2013), as well as their feelings of connection to the school (Bradshaw et al., 2013b; O’Brennan et al., 2014). There is research to suggest that professional development can have a positive effect on teacher efficacy with respect to increasing teachers’ willingness to intervene in bullying incidents (Bell et al., 2010). Nevertheless, it is clear that more work is needed to better understand ways that educators can bridge with students to improve prevention and intervention in bullying situations.
Teachers are not the only adults working in schools or outside of schools who have a role to play in bullying prevention (see Box 5-1). There is emerging research on the important, but often overlooked, group of education support professionals (ESPs), including bus drivers, cafeteria workers, and other paraprofessionals, in bullying prevention (Bradshaw et al., 2013b). The U.S. Department of Education’s Office of Safe and Healthy Students provides guidance on how bus drivers can effectively respond to and prevent bullying (U.S. Department of Health and Human Services,
2015). These individuals are rarely provided training in bullying prevention and their school’s policies related to bullying. They are seldom engaged in schoolwide bullying prevention efforts, despite witnessing rates of student bullying similar to teachers.
School resource officers (SROs) are also an increasing presence in schools (James and McCallion, 2013), but their engagement in prevention programming is rare. Most SROs are engaged primarily in law enforcement–related activities, such as patrolling school grounds, responding to crime/disorder reports, and investigating leads about crime (Coon and Travis III, 2012; James et al., 2011). The SRO role is traditionally viewed as a triad of law enforcement, teacher, and counselor, so it makes sense that an officer can play a potentially important role on school safety teams and in bullying prevention efforts. However, few studies have examined their role in implementing anti-bullying policies and interventions (James and McCallion, 2013; Robles-Piña and Denham, 2012). The limited research on this topic acknowledges a tension between two different perspectives. The first is that SROs should not be involved in bullying interventions because many acts that individuals report as bullying are not criminal matters (Broll and Huey, 2015; Parr et al., 2012). In contrast, others view the SRO as not just a sworn law enforcement officer but also an important member of the school staff who can and should be trained to engage in teaching- and counselor-related activities (Coon and Travis III, 2012; Robles-Piña and Denham, 2012). Although SROs are often called in when there is a problem, additional research is needed on how best to leverage their expertise and role to promote a positive school climate and prevent bullying.
The Role of Parents
Not surprisingly, parents play an important role in helping youth navigate social challenges and adapting to stress (Collins et al., 2000). There is a large and growing body of research documenting the efficacy and effectiveness of preventive interventions that involve parents, particularly at the selective and indicated levels. However, the vast majority of these programs focus on youth violence prevention, social-emotional development, and academic outcomes, with virtually no RCT-design evaluations of programs that were developed specifically to prevent bullying. Yet, intervention research consistently highlights the importance of parents in shaping positive outcomes for youth. The meta-analysis by Ttofi and Farrington (2009) found that several family factors were important elements of effective bullying prevention programs, including parent training and informing parents about bullying. However, few of the evaluations of universal programs reviewed by the committee collected comprehensive data on the penetration or uptake of those parent-focused elements. For example, sending home
information to parents and offering workshops is much easier than ensuring parents’ engagement, program attendance, and actual use of those materials (Bradshaw et al., 2009b). It is quite possible that parent-focused programming for school-age youth is more efficient and effective at the selective and indicated levels than at the universal level (Arseneault et al., 2010).
The notion that “violence begets violence” also applies to the need for interventions targeted to individuals who bully and are bullied by others. Espelage and colleagues (2012) examined the relationship between peer victimization and family violence in early adolescence and found that youth
who were identified as poly-victims9 or who reported relational bullying were more likely to also endorse witnessing domestic violence and being physically or sexually abused at home when compared to nonvictimized youth. Similarly, parents also need to be wary of behavior akin to bullying in the home, such as among siblings or cousins (Jones et al., 2013), which speaks to the need for increased parent awareness of the signs and symptoms of bullying and its impact on the youth and family.
Hawley and Williford (2015) specifically called for the active and consistent involvement of parents in anti-bullying interventions, particularly with respect to the prevention of cyberbullying. In a study of late adolescent victims of bullying, Hemphill and colleagues (2014) found that having opportunities for prosocial involvement in the family lessened subsequent involvement in nonviolent antisocial behaviors. Wang and colleagues (2009) also found that parental support may protect adolescents from multiple forms of bullying, including cyberbullying, which makes parental involvement a potentially critical intervention target.
Health Care Professionals and Bullying Prevention and Intervention
Health care clinicians, including mental and behavioral health experts, can be important players in bullying prevention, especially when they can collaborate with teachers and other education professionals. Evidence of the physical, mental, and behavioral health issues of children who bully, are bullied, or observe bullying incidents (Borowsky et al., 2013; Vessey et al., 2013; Wolke and Lereya, 2015) provides child health and mental health clinicians in community and acute care settings with knowledge to engage in bullying prevention interventions.
Child health care providers can address biological and psychological consequences of bullying in many ways (Fekkes, 2006). Although their clinical roles and responsibilities may vary, community- and hospital-based child health care providers have opportunities to identify and support children, family members, and school personnel in need of care or advice. In addition to physicians and nurses, other health care providers, such as psychologists, dentists, social workers, physical therapists, occupational therapists, and speech and language professionals, may encounter children and youth who have been bullied, who bully, or who have been bystanders to bullying incidents.
Bullying raises complex issues for health care providers because of the associations among bullying and many physical, emotional, behavioral, and social issues such as depression, anxiety, suicide, psychosomatic complaints,
___________________
9 The term “poly-victim” for individuals who experience multiple types of victimization is discussed in Chapter 4.
substance abuse, school truancy and delinquency (Borowsky et al., 2013; Dale et al., 2014; Gini and Pozzoli, 2009). Clinicians in schools, clinics, primary care practices, schools, and school-based health centers have opportunities to discuss bullying during visits for well-child care, annual school or sports exams, and routine acute care (Magalnick and Mazyck, 2008). Because middle school students experience higher rates of being bullied than students in high school (Robers et al., 2015), encounters with early adolescents might be especially important for prevention and anticipatory guidance. Because of possible long-term effects of bullying (and other early childhood adversity or toxic stresses) (Lereya et al., 2015; Shonkoff et al., 2012), youth in high school might have emotional or mental health issues that relate to previous bullying incidents.
In addition to children and youth who have been bullied, those who bully may have specific health care needs. They might have family situations that are characterized by violence, abuse, neglect, low socioeconomic status, or other stressful issues. Perpetrating bullying might be the manifestation of other underlying issues, such as mental or behavioral health problems, alienation, homelessness, or undetected learning disabilities.
Because some children internalize victimization or emotional difficulties (Adams et al., 2013; Borowsky et al., 2013), the physical or emotional impacts of bullying on children who bully, have been bullied, or have been bystanders to bullying might not be readily apparent to family members, educators, or health care professionals. Therefore, during child health encounters, clinicians might inquire about changes in behavior, appetite, and sleep and about children’s attitudes toward school as ways of screening for involvement with bullying.
Given possible somatization of symptoms among children who have been bullied (Gini and Pozzoli, 2009), health care professionals who see children for purported acute care problems that don’t show evidence of illness might consider experience of being bullied among many other possible reasons for the symptoms claimed for the visit or for parents’ or children’s concerns. Children and youth with certain diagnoses and conditions might be at higher risk for being targets of bullying than others. This includes children with chronic illnesses (e.g., diabetes, obesity, or cerebral palsy), autism spectrum disorders, attention deficit disorders, learning disabilities, congenital anomalies, and behavioral or emotional illnesses (Adams et al., 2013; Pittet et al., 2009; Storch et al., 2006; Twyman et al., 2010).
Health care professionals might also consider protective factors for youth involved with bullying and could provide guidance to parents and children regarding the importance of certain supports. For example, parent connectedness and perceived caring by friends and nonparental adults can be protective factors for some children and youth involved with bullying (Borowsky et al., 2013).
Because most bullying occurs at school (Robers et al., 2015), school nurses are often on the frontlines of caring for children and youth involved in bullying. They might be the first health care professional involved with children and youth who have been bullied in school settings, especially some groups of children who are particularly at risk. As noted above, counselors are often called upon to respond to bullying prevention situations, but they rarely use evidence-based bullying-intervention approaches when providing counseling services to youth who bully or who are victims of bullying. Additional research is needed on the selective and indicated mental health interventions referenced above (e.g., CBITS, MST, FFT, Wraparound/Case Management), as they, too, may be effective for youth involved in bullying. Moreover clinicians should inquire about bullying, even when the youth presents with symptoms that seem consistent with other mental health problems, as bullying may be a contributing factor.
Bullying prevention intervention presents inherent challenges to pediatric health care providers. For example, if a health care professional suspects or identifies a child who has been involved with bullying, effective mechanisms for referral and collaboration with education and other professionals are typically lacking. Appropriate counseling or other services may be in short supply in communities, especially in remote rural areas or other underserved areas. Sharing patient or student information across settings presents legal and logistical challenges. Involvement of parents may be difficult. Reporting mechanisms under state and local laws and other policies might not pertain to situations in which a child health professional detects that bullying has occurred. Finally, best practices or procedures for follow-up by health care professionals are lacking from the evidence-based literature.
Other challenges reside in integrating bullying prevention intervention into the daily responsibilities and realities of health care professionals, regardless of setting. Mechanisms to compensate for time spent on screening, referral, counseling, follow-up of bullying incidents among patients and school or community education may lack public or private sources of financing and reimbursement.
Organizations such as the American Academy of Pediatrics and the National Association of School Nurses have issued statements on the bullying prevention role of their respective members (Committee on Injury, Violence, and Poison Prevention, 2009; DeSisto and Smith, 2015). Interdisciplinary collaboration in this area and identification of effective intervention for best child health outcomes need further study.
The Role of Media
As noted in previous sections of this report, the media serves as both a positive and negative influence on youth with respect to bullying behavior.
There are relatively few RCT studies of social norm campaigns focused on bullying awareness and prevention, despite the large body of public health research suggesting such approaches may be effective at shifting norms, attitudes, and behavior (Wakefield et al., 2010). For example, there have been programs that have delivered normative information as a primary tool for changing socially significant behaviors, such as alcohol consumption (Neighbors et al., 2004), tobacco and drug use (Donaldson et al., 1994), and gambling (Larimer and Neighbors, 2003). Additional work is clearly needed to better understand both the risks and the opportunities associated with media-focused campaigns and social norms–based interventions in relation to bullying.
Social Media
Social media offers both intervention challenges and opportunities for cyberbullying. A challenge is that social media provides a platform on which bullying can occur. This may include bullying by private messages sent within a site, by posting public and embarrassing content about a peer, or by creating a “false” profile of the target and posting embarrassing or untruthful content. Because of the multimedia capacity of these sites, embarrassing content may include text, photos, or even video. Social media allows this content to be spread rapidly within a network, as well as shared through others’ networks. Even if the original post is removed, content that has been shared may be difficult to locate and remove.
Social media also provides opportunities to prevent and intervene with bullying. Organizations dedicated to intervention for preventing and treating consequences of bullying may use social media to maintain a presence in those electronic communities where bullying is taking place and to use their platforms for positive messages. Social media may be used to promote prevention messages, such as the It Gets Better campaign,10 although the committee recognizes that this use of social media, as well as many other intervention approaches, needs further evaluation to determine if it helps or harms children involved in bullying. Social media may also provide opportunities for those who have experienced bullying to directly communicate with an organization. While limited studies have evaluated these efforts, the platform of social media provides opportunities to test the effectiveness of these approaches.
___________________
10 The It Gets Better Program employs user-generated media to reach LGBT youth and ameliorate depression and suicidal thoughts among these individuals during their adolescent years. See http://www.itgetsbetter.org [April 2016].
SUMMARY
Systematic reviews and meta-analyses over the past decade recommend that the most likely effective bullying prevention programs are whole school, multicomponent programs that combine elements of universal and targeted strategies (Bradshaw, 2015; Rigby and Slee, 2008; Vreeman and Carroll, 2007). Yet, most meta-analyses of bullying programs show mixed effects and small to moderate effect sizes, at best. When the effects are positive, they are more likely to be effects on attitudes, knowledge, and perceptions, rather than effects on bullying behavior such as experience as a perpetrator or target of bullying. If a universal program does include elements intended to reduce related risk factors or enhance protective factors such as social competence, these elements tend to be embedded in the program so that it is not easy to discern which program components produce desired results for bullying-related behavior. The effects of preventive interventions tend to be greatest for the highest-risk youth, even for interventions in early elementary school (Bradshaw et al., 2015; Limbos et al., 2007; Petras et al., 2008).
Few bullying programs include specific intervention components for youth at risk for involvement in bullying or for youth already involved in bullying, whether as perpetrators or targets (or both). Other school-based interventions tend to target behaviors associated with bullying (e.g., aggressive behavior, social skill development) or the mental health problems associated with being buillied (depression, anxiety, academic failure). Few of the selective and indicated preventive interventions for identified perpetrators (aggressive youth) or targets (youth with mental health issues or at risk for suicide) are school-based, so there needs to be stronger connections between schools, families, and community-based treatment programs. Moreover, these programs need to be further evaluated with regard to impacts on bullying behavior, as they were originally developed to address violence and mental health problems. Yet, many of these problems co-occur and have overlapping risk and protective factors, which suggests these other evidence-based selective and indicated violence prevention models may also demonstrate positive effects for youth involved in bullying.
There is still a dearth of intervention research on programs related to cyberbullying and on programs targeted to vulnerable populations such as LGBT youth, youth with chronic health problems, or youth with developmental disabilities such as autism (Minton, 2014). The role of peers in interventions for at-risk students or for those who are perpetrators or targets needs further clarification, whether that is for peers as bystanders or peers as interventionists, or peers as fellow perpetrators, or targets. Despite increasing interest in programs aimed at increasing equity, shifting norms related to stereotypes, or the use of restorative practices, there are
few fully developed models that target these issues, and virtually no randomized studies documenting outcomes associated with these approaches. Additional work is needed on these models to determine whether broader dissemination of these approaches is warranted.
Schools may want to consider implementing a multicomponent program that focuses on school climate, positive behavior support, social and emotional learning, or violence prevention more generally, rather than implementing a bullying-specific preventive intervention, as these more inclusive programs may reach a broader set of outcomes for students and the school environment. Tiered preventive interventions appear to be a promising model for schools, but the lack of rigorously tested selective and indicated preventive interventions focused specifically on bullying means that other violence and mental health prevention models should be leveraged and integrated to increase efficiency. Regardless of the model selected, issues related to implementation fidelity, spanning initial buy-in, and adoption through sustainability, need careful consideration and an authentic investment of resources in order to achieve outcomes.
FINDINGS AND CONCLUSIONS
Findings
Finding 5.1: The most likely effective bullying prevention programs are whole school, multicomponent programs that combine elements of universal and targeted strategies.
Finding 5.2: The findings from meta-analyses of bullying prevention programs have been mixed, with the largest effects observed for whole school programs implemented in Europe, as compared to programs tested in the United States. The challenge of designing and delivering effective bullying prevention programs in the United States may be due to the greater social and economic complexities, including greater income disparities and racial/ethnic heterogeneity in the United States, compared with European countries. More research is needed in the United States focusing on developing and testing novel models for bullying prevention programming and the identification of strategies for increasing fidelity of implementation and effect sizes.
Finding 5.3: Research on the role of peers in bullying prevention interventions has been mixed, with some studies suggesting the need for more peer-based interventions, such as friendship-making components, and others calling for more caution because peer-based interventions have produced null or even iatrogenic effects.
Finding 5.4: Few bullying programs include specific intervention components for youth at risk for bullying (e.g., ethnic minorities, sexual minorities, youth with disabilities), or for youth already involved in bullying as perpetrators or targets (or both), and the studies examining impacts of bullying prevention programs for these subpopulations are rare.
Finding 5.5: Few of the selective and indicated preventive interventions for identified perpetrators (aggressive youth) or targets (e.g., bullied youth with mental health issues or at risk for suicide) are school-based, so there needs to be stronger connections among schools, families, and community-based treatment programs.
Finding 5.6: There is a growing interest in research documenting the effectiveness of bullying and youth violence preventive interventions that involve parents, particularly at the selective and indicated levels. However, to date few such family-focused programs have been developed or tested in relation to impacts specifically on bullying.
Finding 5.7: There is emerging international research that suggests a variety of models may be effective at reducing both cyberbullying and traditional bullying.
Conclusions
Conclusion 5.1: The vast majority of research on bullying prevention programming has focused on universal school-based programs; however, the effects of those programs within the United States appear to be relatively modest. Multicomponent schoolwide programs appear to be most effective at reducing bullying and should be the types of programs implemented and disseminated in the United States.
Conclusion 5.2: Most of the school, family, and community-based prevention programs tested using randomized controlled trial designs have focused on youth violence, delinquency, social-emotional development, and academic outcomes, with limited consideration of the impacts on bullying specifically. However, it is likely that these programs also produce effects on bullying, which have largely been unmeasured and therefore data on bullying outcomes should be routinely collected in future research.
Conclusion 5.3: There has been limited research on selective and indicated models for bullying intervention programming, either inside or
outside of schools. More attention should be given to these interventions in future bullying research.
Conclusion 5.4: The extant, empirically supported selective and indicated preventive interventions for violence and delinquency should also be leveraged to meet the needs of students involved in bullying, or those experiencing the mental and behavioral health consequences of bullying. These programs should be integrated into a multi-tiered system of supports for students at risk for engaging in or experiencing the consequences of bullying.
Conclusion 5.5: The role of peers in bullying prevention as bystanders and as intervention program leaders needs further clarification and empirical investigation in order to determine the extent to which peer-led programs are effective and robust against potentially iatrogenic effects.
Conclusion 5.6: The role of online resources or social marketing campaigns in bullying prevention or intervention needs further clarification and empirical investigation in order to determine whether these resources and programs are effective.
Conclusion 5.7: Since issues of power and equity are highly relevant to bullying, fully developed prevention models that target these issues as an approach for preventing bullying should be conducted using randomized controlled trial designs.
Conclusion 5.8: Additional research is needed on the effectiveness of programs targeted to vulnerable populations such as lesbian, gay, bisexual, and transgender youth, youth with chronic health problems such as obesity, or those with developmental disabilities (e.g., autism), as well as variation in the effectiveness of universal programs for these subpopulations.
Conclusion 5.9: There is a strong need for additional programming and effectiveness research on interdisciplinary collaboration with health care practitioners, parents, school resource officers, community-based organizations (e.g., scouts, athletics), and industry to address issues related to bullying and cyberbullying.
Conclusion 5.10: Regardless of the prevention program or model selected, issues related to implementation fidelity, spanning initial buy-in and adoption through taking programs to scale and sustainability, need
careful consideration and an authentic investment of resources in order to achieve outcomes and sustained implementation.
REFERENCES
Adams, R.E., Fredstrom, B.K., Duncan, A.W., Holleb, L.J., and Bishop, S.L. (2013). Using self- and parent-reports to test the association between peer victimization and internalizing symptoms in verbally fluent adolescents with ASD. Journal of Autism and Developmental Disorders, 44(4), 861-872.
Afterschool Alliance. (2014). America after 3 pm: Afterschool Programs in Demand. Available: http://www.afterschoolalliance.org/documents/AA3PM-2014/AA3PM_Key_Findings.pdf [December 2015].
Ahtola, A., Haataja, A., Kärnä, A., Poskiparta, E., and Salmivalli, C. (2012). For children only? Effects of the KiVa Anti-Bullying Program on teachers. Teaching and Teacher Education, 28(6), 851-859.
Ajzen, I. (1985). From intentions to actions: A theory of planned behavior. In J. Kuh and J. Beckmann (Eds.), Action Control: From Cognition to Behavior (pp. 11-39). Berlin: Springer-Verlag.
Aos, S., Lee, S., Drake, E., Pennucci, A., Klima, T., Miller, M., Anderson, L., Mayfield, J., and Burley, M. (2011). Evidence-based Options to Improve Statewide Outcomes, July 2011 Update (Pub. No. 04-07-3901). Olympia: Washington State Institute for Public Policy. Available: http://wsipp.wa.gov/pub.asp [December 2015].
Arseneault, L., Bowes, L., and Shakoor, S. (2010). Bullying victimization in youths and mental health problems: “Much ado about nothing”? Psychological Medicine, 40(05), 717-729.
Bagley, C., and Pritchard, C. (1998). The reduction of problem behaviours and school exclusion in at-risk youth: An experimental study of school social work with cost-benefit analyses. Child and Family Social Work, 3(4), 219-226.
Barnes, T.N., Smith, S.W., and Miller, M.D. (2014). School-based cognitive-behavioral interventions in the treatment of aggression in the United States: A meta-analysis. Aggression and Violent Behavior, 19(4), 311-321.
Barrera Jr, M., Biglan, A., Taylor, T.K., Gunn, B.K., Smolkowski, K., Black, C., Ary, D.V., and Fowler, R.C. (2002). Early elementary school intervention to reduce conduct problems: A randomized trial with Hispanic and non-Hispanic children. Prevention Science, 3(2), 83-94.
Batsche, G. (2014). Multi-tiered system of supports for inclusive schools. In J. McLeskey, N.L. Waldron, F. Sponder, and B. Algozzine (Eds.) Handbook of Effective Inclusive Schools: Research and Practice (pp. 183-196). New York: Routledge.
Baughman-Sladky, M., Hussey, D., Flannery, D., and Jefferis, E. (2015). Adolescent delinquency and violent behavior. In T.P. Gullotta, R.W. Plant, and M.A. Evans (Eds.), Handbook of Adolescent Behavioral Problems: Evidence-Based Approaches to Prevention and Treatment, Second Edition (pp. 445-471). New York: Springer Press.
Bauman, S., Rigby, K., and Hoppa, K. (2008). U.S. teachers’ and school counsellors’ strategies for handling school bullying incidents. Educational Psychology, 28(7), 837-856.
Beets, M.W., Flay, B.R., Vuchinich, S., Acock, A.C., Li, K.-K., and Allred, C. (2008). School climate and teachers’ beliefs and attitudes associated with implementation of the Positive Action Program: A diffusion of innovations model. Prevention Science, 9(4), 264-275.
Bell, C.D., Raczynski, K.A., and Horne, A.M. (2010). Bully Busters Abbreviated: Evaluation of a group-based bully intervention and prevention program. Group Dynamics: Theory, Research, and Practice, 14(3), 257-267.
Berguno, G., Leroux, P., McAinsh, K., and Shaikh, S. (2004). Children’s experience of loneliness at school and its relation to bullying and the quality of teacher interventions. The Qualitative Report, 9(3), 483-499.
Berry, K., and Hunt, C.J. (2009). Evaluation of an intervention program for anxious adolescent boys who are bullied at school. Journal of Adolescent Health, 45(4), 376-382.
Biggs, B.K., Vernberg, E.M., Twemlow, S.W., Fonagy, P., and Dill, E.J. (2008). Teacher adherence and its relation to teacher attitudes and student outcomes in an elementary school–based violence prevention program. School Psychology Review, 37(4), 533.
Biglan, A., Flay, B.R., and Wagenaar, A.C. (2015). Commentary on the 2015 SPR Standards of Evidence. Prevention Science, 16(7), 927-932.
Borowsky, I.W., Taliaferro, L.A., and McMorris, B.J. (2013). Suicidal thinking and behavior among youth involved in verbal and social bullying: Risk and protective factors. Journal of Adolescent Health, 53(1), S4-S12.
Botvin, G.J., Griffin, K.W., and Nichols, T.D. (2006). Preventing youth violence and delinquency through a universal school-based prevention approach. Prevention Science, 7(4), 403-408.
Bowes, L., Maughan, B., Caspi, A., Moffitt, T., and Arseneault, L. (2010). Families promote emotional and behavioural resilience to bullying: Evidence of an environmental effect. Child Psychology and Psychiatry, 51(7), 809-817.
Bradshaw, C.P. (2013). Preventing bullying through Positive Behavioral Interventions and Supports (PBIS): A multitiered approach to prevention and integration. Theory into Practice, 52(4), 288-295.
Bradshaw, C.P. (2015). Translating research to practice in bullying prevention. American Psychologist, 70(4), 322.
Bradshaw, C.P. (Ed.). (in press). Handbook of Bullying Prevention: A Life Course Perspective: Washington, DC: National Association of Social Workers Press.
Bradshaw, C.P., and Waasdorp, T.E. (2009). Measuring and changing a “culture of bullying.” School Psychology Review, 38(3), 356-361.
Bradshaw, C.P., Koth, C.W., Bevans, K.B., Ialongo, N., and Leaf, P.J. (2008). The impact of school-wide Positive Behavioral Interventions and Supports (PBIS) on the organizational health of elementary schools. School Psychology Quarterly, 23(4), 462-473.
Bradshaw, C.P., Sawyer, A.L., and O’Brennan, L.M. (2009a). A social disorganization perspective on bullying-related attitudes and behaviors: The influence of school context. American Journal of Community Psychology, 43(3-4), 204-220.
Bradshaw, C.P., Koth, C.W., Thornton, L.A., and Leaf, P.J. (2009b). Altering school climate through school-wide Positive Behavioral Interventions and Supports: Findings from a group-randomized effectiveness trial. Prevention Science, 10(2), 100-115.
Bradshaw, C.P., Zmuda, J.H., Kellam, S.G., and Ialongo, N.S. (2009c). Longitudinal impact of two universal preventive interventions in first grade on educational outcomes in high school. Journal of Educational Psychology, 101(4), 926-937.
Bradshaw, C.P., Mitchell, M.M., and Leaf, P.J. (2010). Examining the effects of schoolwide Positive Behavioral Interventions and Supports on student outcomes: Results from a randomized controlled effectiveness trial in elementary schools. Journal of Positive Behavior Interventions, 12(3), 133-148.
Bradshaw, C.P., Waasdorp, T.E., and Leaf, P.J. (2012). Effects of school-wide Positive Behavioral Interventions and Supports on child behavior problems. Pediatrics, 130(5), e1136-e1145.
Bradshaw, C.P., Waasdorp, T.E., Goldweber, A., and Johnson, S.L. (2013a). Bullies, gangs, drugs, and school: Understanding the overlap and the role of ethnicity and urbanicity. Journal of Youth and Adolescence, 42(2), 220-234.
Bradshaw, C.P., Waasdorp, T.E., O’Brennan, L.M., and Gulemetova, M. (2013b). Teachers’ and education support professionals’ perspectives on bullying and prevention: Findings from a National Education Association study. School Psychology Review, 42(3), 280-297.
Bradshaw, C.P., Bottiani, J.H., Osher, D., and Sugai, G. (2014a). The integration of positive behavioral interventions and supports and social and emotional learning. In M.D. Weist, N.A. Lever, and J.S. Owens (Eds.), Handbook of School Mental Health (pp. 101-118). New York: Springer.
Bradshaw, C.P., Debnam, K., Johnson, S., Pas, E., Hershfeldt, P., Alexander, A., Barrett, S., and Leaf, P. (2014b). Maryland’s evolving system of social, emotional, and behavioral interventions in public schools: The Maryland Safe and Supportive Schools project. Adolescent Psychiatry, 4(3), 194-206.
Bradshaw, C.P., Waasdorp, T.E., and Leaf, P.J. (2015). Examining variation in the impact of school-wide Positive Behavioral Interventions and Supports: Findings from a randomized controlled effectiveness trial. Journal of Educational Psychology, 107(2), 546-557.
Broll, R., and Huey, L. (2015). “Just being mean to somebody isn’t a police matter”: Police perspectives on policing cyberbullying. Journal of School Violence, 14(2), 155-176.
Brown, E.C., Low, S., Smith, B.H., and Haggerty, K.P. (2011). Outcomes from a school-randomized controlled trial of Steps to Respect: A bullying prevention program. School Psychology Review, 40(3), 423-443.
Bruns, E.J., Burchard, J.D., and Yoe, J.T. (1995). Evaluating the Vermont system of care: Outcomes associated with community-based Wraparound services. Journal of Child and Family Studies, 4(3), 321-339.
Bulanda, J.J., Bruhn, C., Byro-Johnson, T., and Zentmyer, M. (2014). Addressing mental health stigma among young adolescents: Evaluation of a youth-led approach. Health & Social Work, 39(2), 73-80.
Carney, M.M., and Buttell, F. (2003). Reducing juvenile recidivism: Evaluating the Wraparound services model. Research on Social Work Practice, 13(5), 551-568.
Catalano, R.F., Mazza, J.J., Harachi, T.W., Abbott, R.D., Haggerty, K.P., and Fleming, C.B. (2003). Raising healthy children through enhancing social development in elementary school: Results after 1.5 years. Journal of School Psychology, 41(2), 143-164.
Chaux, E., Velasquez, A.M., Schultze-Krumbholz, A., and Scheithauer, H. (2016). Effects of the cyberbullying prevention program Media Heroes (Medienhelden) on traditional bullying. Aggressive Behavior, 42(2), 157-165.
Cohen, J.A., Deblinger, E., Mannarino, A.P., and Steer, R.A. (2004). A multisite, randomized controlled trial for children with sexual abuse–related PTSD symptoms. Journal of the American Academy of Child & Adolescent Psychiatry, 43(4), 393-402.
Cohen, J.A., Mannarino, A.P., and Knudsen, K. (2005). Treating sexually abused children: 1-year follow-up of a randomized controlled trial. Child Abuse & Neglect, 29(2), 135-145.
Cohen, J., Mannarino, A., and Deblinger, E. (2006). Treating Trauma and Traumatic Grief in Children and Adolescents. New York: Guilford Press.
Collins, W.A., Maccoby, E.E., Steinberg, L., Hetherington, E.M., and Bornstein, M.H. (2000). Contemporary research on parenting: The case for nature and nurture. American Psychologist, 55(2), 218-232.
Committee on Injury, Violence, and Poison Prevention. (2009). Policy statement—Role of the pediatrician in youth violence prevention. Pediatrics, 124(1), 393-402.
Conduct Problems Prevention Research Group. (1999). Initial impact of the Fast Track prevention trial for conduct problems: II. Classroom effects. Journal of Consulting and Clinical Psychology, 67(5), 648-657.
Conduct Problems Prevention Research Group. (2002). Using the Fast Track randomized prevention trial to test the early-starter model of the development of serious conduct problems. Development and Psychopathology, 14(4), 925-943.
Conduct Problems Prevention Research Group. (2010). Fast Track intervention effects on youth arrests and delinquency. Journal of Experimental Criminology, 6(2), 131-157.
Conduct Problems Prevention Research Group. (2011). The effects of the Fast Track preventive intervention on the development of conduct disorder across childhood. Child Development, 82(1), 331-345.
Connell, A.M., Dishion, T.J., Yasui, M., and Kavanagh, K. (2007). An adaptive approach to family intervention: Linking engagement in family-centered intervention to reductions in adolescent problem behavior. Journal of Consulting and Clinical Psychology, 75(4), 568-579.
Connolly, J., Josephson, W., Schnoll, J., Simkins-Strong, E., Pepler, D., MacPherson, A., Weiser, J., Moran, M., and Jiang, D. (2015). Evaluation of a youth-led program for preventing bullying, sexual harassment, and dating aggression in middle schools. The Journal of Early Adolescence, 35(3), 403-434.
Coon, J.K., and Travis III, L.F. (2012). The role of police in public schools: A comparison of principal and police reports of activities in schools. Police Practice and Research, 13(1), 15-30.
Cross, D., Shaw, T., Hadwen, K., Cardoso, P., Slee, P., Roberts, C., Thomas, L., and Barnes, A. (2015). Longitudinal impact of the Cyber Friendly Schools program on adolescents’ cyberbullying behavior. Aggressive Behavior, 42(2), 166-180.
Cunningham, C.E., Vaillancourt, T., Cunningham, L.J., Chen, Y., and Ratcliffe, J. (2011). Modeling the bullying prevention program design recommendations of students from grades five to eight: A discrete choice conjoint experiment. Aggressive Behavior, 37(6), 521-537.
Dale, J., Russell, R., and Wolke, D. (2014). Intervening in primary care against childhood bullying: An increasingly pressing public health need. Journal of the Royal Society of Medicine, 107(6), 219-223.
Deblinger, E., Mannarino, A.P., Cohen, J.A., Runyon, M.K., and Steer, R.A. (2011). Trauma-focused cognitive behavioral therapy for children: Impact of the trauma narrative and treatment length. Depression and Anxiety, 28(1), 67-75.
Del Rey, R., Casas, J.A., and Ortega, R. (2015). The impacts of the ConRed program on different cyberbulling roles. Aggressive Behavior, 42(2), 123-135.
DeRosier, M.E. (2004). Building relationships and combating bullying: Effectiveness of a school-based social skills group intervention. Journal of Clinical Child & Adolescent Psychology, 33(1), 196-201.
DeRosier, M.E., and Marcus, S.R. (2005). Building friendships and combating bullying: Effectiveness of S.S.GRIN at one-year follow-up. Journal of Clinical Child & Adolescent Psychology, 34(1), 140-150.
DeSisto, M.C., and Smith, S. (2015). Bullying prevention in schools: Position statement. National Association of School Nurses, 30(3), 189-191.
Dishion, T.J., and Kavanagh, K. (2003). Intervening in Adolescent Problem Behavior: A Family-centered Approach. New York: Guilford Press.
Dishion, T.J., Brennan, L.M., Shaw, D.S., McEachern, A.D., Wilson, M.N., and Jo, B. (2014). Prevention of problem behavior through annual family check-ups in early childhood: Intervention effects from home to early elementary school. Journal of Abnormal Child Psychology, 42(3), 343-354.
Doane, A.N., Kelley, M.L., and Pearson, M.R. (2015). Reducing cyberbullying: A Theory of Reasoned Action-based video prevention program for college students. Aggressive Behavior, 42(2), 136-146.
Dodge, K., Bierman, K., Coie, J., Greenberg, M., Lochman, J., McMahon, R., and Pinderhughes, E. (2015). Impact of early intervention on psychopathology, crime, and well-being at age 25. The American Journal of Psychiatry, 172(1), 59-70.
Dodge, K.A., Dishion, T.J., and Lansford, J.E. (2006). Deviant peer influences in intervention and public policy for youth. Society for Research in Child Development, 20(1) 1-19.
Domitrovich, C.E., Bradshaw, C.P., Poduska, J.M., Hoagwood, K., Buckley, J.A., Olin, S., Romanelli, L.H., Leaf, P.J., Greenberg, M.T., and Ialongo, N.S. (2008). Maximizing the implementation quality of evidence-based preventive interventions in schools: A conceptual framework. Advances in School Mental Health Promotion, 1(3), 6-28.
Domitrovich, C.E., Bradshaw, C.P., Greenberg, M.T., Embry, D., Poduska, J.M., and Ialongo, N.S. (2010). Integrated models of school-based prevention: Logic and theory. Psychology in the Schools, 47(1), 71-88.
Domitrovich, C.E., Bradshaw, C.P., Berg, J., Pas, E., Becker, K., Musci, R., Embry, D., and Ialongo, N. (2016). How do school-based prevention programs impact teachers? Findings from a randomized trial of an integrated classroom management and social-emotional program. Prevention Science, 17, 325-337.
Donaldson, S.I., Graham, J.W., and Hansen, W.B. (1994). Testing the generalizability of intervening mechanism theories: Understanding the effects of adolescent drug use prevention interventions. Journal of Behavioral Medicine, 17(2), 195-216.
Duong, J., and Bradshaw, C.P. (2013). Using the extended parallel process model to examine teachers’ likelihood of intervening in bullying. Journal of School Health, 83(6), 422-429.
Duong, J., and Bradshaw, C.P. (2015). Bullying and suicide prevention: Taking a balanced approach that is scientifically informed. In P. Goldblum, D.L. Espelage, J. Chu, and B. Bongar (Eds.), Youth Suicide and Bullying: Challenges and Strategies for Prevention and Intervention (pp. 19-27). New York: Oxford University Press.
Durlak, J., Weissberg, R., Taylor, R., and Dymnicki, A. (2007). The Effects of School-based Social and Emotional Learning: A Meta-analytic Review. Unpublished manuscript, Loyola University, Chicago, IL.
Durlak, J.A., Weissberg, R.P., and Pachan, M. (2010). A meta-analysis of after-school programs that seek to promote personal and social skills in children and adolescents. American Journal of Community Psychology, 45(3-4), 294-309.
Durlak, J.A., Weissberg, R.P., Dymnicki, A.B., Taylor, R.D., and Schellinger, K.B. (2011). The impact of enhancing students’ social and emotional learning: A meta-analysis of school-based universal interventions. Child Development, 82(1), 405-432.
Eddy, J.M., Reid, J.B., and Fetrow, R.A. (2000). An elementary school-based prevention program targeting modifiable antecedents of youth delinquency and violence: Linking the Interests of Families and Teachers (LIFT). Journal of Emotional and Behavioral Disorders, 8(3), 165-176.
Elgar, F.J., Napoletano, A., Saul, G., Dirks, M.A., Craig, W., Poteat, V.P., Holt, M., and Koenig, B.W. (2014). Cyberbullying victimization and mental health in adolescents and the moderating role of family dinners. JAMA Pediatrics, 168(11), 1015-1022.
Embry, D.D., Flannery, D.J., Vazsonyi, A.T., Powell, K.E., and Atha, H. (1996). Peacebuilders: A theoretically driven, school-based model for early violence prevention. American Journal of Preventive Medicine, 12(5), 91-100.
Eron, L., Huesmann, R., Spindler, A., Guerra, N., Henry, D., and Tolan, P. (2002). A cognitive-ecological approach to preventing aggression in urban settings: Initial outcomes for high-risk children. Journal of Consulting and Clinical Psychology, 70(1), 179-194.
Espelage, D.L., and Swearer, S.M. (2008). Current perspectives on linking school bullying research to effective prevention strategies. In T.W. Miller (Ed.), School Violence and Primary Prevention (pp. 335-353). New York: Springer Science + Business Media.
Espelage, D.L., Gutgsell, E.W., and Swearer, S.M. (2004). Bullying in American Schools: A Social-ecological Perspective on Prevention and Intervention. Mahwah, NJ: L. Erlbaum Associates.
Espelage, D.L., Low, S., and De La Rue, L. (2012). Relations between peer victimization subtypes, family violence, and psychological outcomes during early adolescence. Psychology of Violence, 2(4), 313-324.
Espelage, D.L., Low, S., Polanin, J.R., and Brown, E.C. (2013). The impact of a middle school program to reduce aggression, victimization, and sexual violence. Journal of Adolescent Health, 53(2), 180-186.
Evans, C.B., Fraser, M.W., and Cotter, K.L. (2014). The effectiveness of school-based bullying prevention programs: A systematic review. Aggression and Violent Behavior, 19(5), 532-544.
Farrington, D.P., and Ttofi, M. (2009). School-based programs to reduce bullying and victimization: A systematic review. Campbell Systematic Reviews, 5(6), 1-148.
Farrington, D.P., and Ttofi, M.M. (2011). Bullying as a predictor of offending, violence, and later life outcomes. Criminal Behaviour and Mental Health, 21(2), 90-98.
Fast, J., Fanelli, F., and Salen, L. (2003). How becoming mediators affects aggressive students. Children & Schools, 25(3), 161-171.
Fekkes, M. (2006). Do bullied children get ill, or do ill children get bullied? A prospective cohort study on the relationship between bullying and health-related symptoms. Pediatrics, 117(5), 1568-1574.
Finkelhor, D., Turner, H.A., and Hamby, S. (2012). Let’s prevent peer victimization, not just bullying. Child Abuse & Neglect, 36(4), 271-274.
Fixsen, D., Naoom, S., Blasé, K., Friedman, R., and Wallace, F. (2005). Implementation Research: A Synthesis of the Literature (FMHI Pub. No. 231). Tampa: University of South Florida, Louis de la Parte Florida Mental Health Institute.
Flannery, D.J., Vazsonyi, A.T., Liau, A.K., Guo, S., Powell, K.E., Atha, H., Vesterdal, W., and Embry, D. (2003). Initial behavior outcomes for the Peacebuilders Universal School-Based Violence Prevention Program. Developmental Psychology, 39(2), 292-308.
Flannery, D., Hussey, D., and Jefferis, E. (2005). Adolescent delinquency and violent behavior. In T. Gullotta and G.Adams (Eds), Handbook of Adolescent Behavioral Problems: Evidence-Based Approaches to Prevention and Treatment (pp. 415-438). New York: Springer.
Frey, K.S., Nolen, S.B., Edstrom, L.V.S., and Hirschstein, M.K. (2005). Effects of a school-based social–emotional competence program: Linking children’s goals, attributions, and behavior. Journal of Applied Developmental Psychology, 26(2), 171-200.
Frey, K.S., Hirschstein, M.K., Edstrom, L.V., and Snell, J.L. (2009). Observed reductions in school bullying, nonbullying aggression, and destructive bystander behavior: A longitudinal evaluation. Journal of Educational Psychology, 101(2), 466-481.
Fung, A.L. (2012). Group treatment of reactive aggressors by social workers in a Hong Kong school setting: A two-year longitudinal study adopting quantitative and qualitative approaches. British Journal of Social Work, 42(8), 1533-1555.
Garandeau, C.F., Poskiparta, E., and Salmivalli, C. (2014). Tackling acute cases of school bullying in the KiVa anti-bullying program: A comparison of two approaches. Journal of Abnormal Child Psychology, 42(6), 981-991.
Gartlehner, G., Hansen, R.A., Nissman, D., Lohr, K.N., and Carey, T.S. (2006). A simple and valid tool distinguished efficacy from effectiveness studies. Journal of Clinical Epidemiology, 59(11), 1125-1126.
Gini, G., and Pozzoli, T. (2009). Association between bullying and psychosomatic problems: A meta-analysis. Pediatrics, 123(3), 1059-1065.
Girl Scouts of the USA. (2015). Volunteer with Girl Scouts Today! Available: http://www.girlscouts.org/content/gsusa/en/adults/volunteer.html [February 2016].
Goncy, E.A., Sutherland, K.S., Farrell, A.D., Sullivan, T.N., and Doyle, S.T. (2014). Measuring teacher implementation in delivery of a bullying prevention program: The impact of instructional and procedural adherence and competence on student responsiveness. Prevention Science, 16(3), 440-450.
Goodman, R. (1997). The Strengths and Difficulties Questionnaire: A research note. Journal of Child Psychology and Psychiatry, 38(5), 581-586.
Gottfredson, G.D., and Gottfredson, D.C. (2001). What schools do to prevent problem behavior and promote safe environments. Journal of Educational and Psychological Consultation, 12(4), 313-344.
Gradinger, P., Yanagida, T., Strohmeier, D., and Spiel, C. (2015). Prevention of cyberbullying and cyber victimization: Evaluation of the ViSC Social Competence Program. Journal of School Violence, 14(1), 87-110.
Greenwood, P.W., and Welsh, B.C. (2012). Promoting evidence-based practice in delinquency prevention at the state level. Criminology & Public Policy, 11(3), 493-513.
Grossman, D.C., Neckerman, H.J., Koepsell, T.D., Liu, P.-Y., Asher, K.N., Beland, K., Frey, K., and Rivara, F.P. (1997). Effectiveness of a violence prevention curriculum among children in elementary school: A randomized controlled trial. Journal of the American Medical Association, 277(20), 1605-1611.
Hahn, R., Fuqua-Whitley, D., Wethington, H., Lowy, J., Crosby, A., Fullilove, M., Johnson, R., Liberman, A., Moscicki, E., and Price, L. (2007). Effectiveness of universal school-based programs to prevent violent and aggressive behavior: A systematic review. American Journal of Preventive Medicine, 33(2), S114-S129.
Hanewinkel, R. (2004). Prevention of bullying in German schools: An evaluation of an antibullying approach. In P.K. Smith, D. Pepler, and K. Rigby (Eds.), Bullying in Schools: How Successful Can Interventions Be? (pp. 81-97). Cambridge, UK: Cambridge University Press.
Hatzenbuehler, M.L., Schwab-Reese, L., Ranapurwala, S.I., Hertz, M.F., and Ramirez, M.R. (2015). Associations between antibullying policies and bullying in 25 states. JAMA Pediatrics, 169(10), e152-e411.
Hawkins, J.D., Catalano, R.F., Kosterman, R., Abbott, R., and Hill, K.G. (1999). Preventing adolescent health-risk behaviors by strengthening protection during childhood. Archives of Pediatrics and Adolescent Medicine, 153(3), 226-234.
Hawkins, J.D., Jenson, J.M., Catalano, R., Fraser, M.W., Shapiro, V., Botvin, G.J., Brown, C.H., Beardslee, W., Brent, D., Leslie, L.K., Rotheram-Borus, M.J., Shea, P., Shih, A., Anthony, E., Bender, K., Haggerty, K.P., Gorman-Smith, E., Casey, E., and Stone, S. (2015). Unleashing the Power of Prevention. Institute of Medicine discussion paper. Available: https://nam.edu/perspectives-2015-unleashing-the-power-of-prevention/ [August 2016].
Hawkins, J.D., Kosterman, R., Catalano, R.F., Hill, K.G., and Abbott, R.D. (2005). Promoting positive adult functioning through social development intervention in childhood: Long-term effects from the Seattle Social Development Project. Archives of Pediatrics and Adolescent Medicine, 159(1), 25-31.
Hawkins, J.D., Oesterle, S., Brown, E.C., Monahan, K.C., Abbott, R.D., Arthur, M.W., and Catalano, R.F. (2011). Sustained decreases in risk exposure and youth problem behaviors after installation of the Communities that Care prevention system in a randomized trial. Archives of Pediatrics and Adolescent Medicine, 166(2), 141-148.
Hawley, P.H., and Williford, A. (2015). Articulating the theory of bullying intervention programs: Views from social psychology, social work, and organizational science. Journal of Applied Developmental Psychology, 37, 3-15.
Healy, K.L., and Sanders, M.R. (2014). Randomized controlled trial of a family intervention for children bullied by peers. Behavior Therapy, 45(6), 760-777.
Hektner, J.M., and Swenson, C.A. (2011). Links from teacher beliefs to peer victimization and bystander intervention: Tests of mediating processes. Journal of Early Adolescence, 32(4), 516-536.
Hemphill, S.A., Tollit, M., and Herrenkohl, T.I. (2014). Protective factors against the impact of school bullying perpetration and victimization on young adult externalizing and internalizing problems. Journal of School Violence, 13(1), 125-145.
Henggeler, S.W. (2011). Efficacy studies to large-scale transport: The development and validation of multisystemic therapy programs. Annual Review of Clinical Psychology, 7, 351-381.
Henggeler, S.W., and Sheidow, A.J. (2012). Empirically supported family-based treatments for conduct disorder and delinquency in adolescents. Journal of Marital and Family Therapy, 38(1), 30-58.
Henggeler, S.W., Pickrel, S.G., and Brondino, M.J. (1999). Multisystemic treatment of substance-abusing and -dependent delinquents: Outcomes, treatment fidelity, and transportability. Mental Health Services Research, 1(3), 171-184.
Holt, M.K., Raczynski, K., Frey, K.S., Hymel, S., and Limber, S.P. (2013). School and community-based approaches for preventing bullying. Journal of School Violence, 12(3), 238-252.
Hong, J.S., and Espelage, D.L. (2012). A review of mixed methods research on bullying and peer victimization in school. Educational Review, 64(1), 115-126.
Horner, R.H., Sugai, G., Smolkowski, K., Eber, L., Nakasato, J., Todd, A.W., and Esperanza, J. (2009). A randomized, wait-list controlled effectiveness trial assessing school-wide positive behavior support in elementary schools. Journal of Positive Behavior Interventions, 11(3), 133-144.
Hussey, D.L., and Flannery, D.J. (2007). Implementing and evaluating school-based primary prevention programs and the importance of differential effects on outcomes. Journal of School Violence, 6(2), 117-134.
Institute of Medicine. (1994). Reducing Risks for Mental Disorders: Frontiers for Preventive Intervention Research. Washington, DC: National Academy Press.
James, N., and McCallion, G. (2013). School Resource Officers: Law Enforcement Officers in Schools. Washington, DC: Congressional Research Service.
James, R.K., Logan, J., and Davis, S.A. (2011). Including school resource officers in school-based crisis intervention: Strengthening student support. School Psychology International, 32(2), 210-224.
Jaycox, L.H., Cohen, J.A., Mannarino, A.P., Walker, D.W., Langley, A.K., Gegenheimer, K.L., Scott, M., and Schonlau, M. (2010). Children’s mental health care following Hurricane Katrina: A field trial of trauma-focused psychotherapies. Journal of Traumatic Stress, 23(2), 223-231.
Jiménez-Barbero, J.A., Ruiz-Hernández, J.A., Llor-Zaragoza, L., Pérez-García, M., and LlorEsteban, B. (2016). Effectiveness of anti-bullying school programs: A meta-analysis. Children and Youth Services Review, 61, 165-175.
Johnson, S.R.L., Finigan, N.M., Bradshaw, C.P., Haynie, D.L., and Cheng, T.L. (2011). Examining the link between neighborhood context and parental messages to their adolescent children about violence. Journal of Adolescent Health, 49(1), 58-63.
Jones, L.M., Mitchell, K.J., and Finkelhor, D. (2013). Online harassment in context: Trends from three Youth Internet Safety Surveys (2000, 2005, 2010). Psychology of Violence, 3(1), 53-69.
Kärnä, A., Voeten, M., Little, T.D., Poskiparta, E., Alanen, E., and Salmivalli, C. (2011a). Going to scale: A nonrandomized nationwide trial of the KiVa antibullying program for grades 1–9. Journal of Consulting and Clinical Psychology, 79(6), 796-805.
Kärnä, A., Voeten, M., Little, T.D., Poskiparta, E., Kaljonen, A., and Salmivalli, C. (2011b). A large-scale evaluation of the KiVa Antibullying Program: Grades 4–6. Child Development, 82(1), 311-330.
Kellam, S.G., Rebok, G.W., Ialongo, N., and Mayer, L.S. (1994). The course and malleability of aggressive behavior from early first grade into middle school: Results of a developmental epidemiologically-based preventive trial. Journal of Child Psychology and Psychiatry, 35(2), 259-282.
Klomek, A.B., Kleinman, M., Altschuler, E., Marrocco, F., Amakawa, L., and Gould, M.S. (2011). High school bullying as a risk for later depression and suicidality. Suicide and Life-Threatening Behavior, 41(5), 501-516.
Koth, C.W., Bradshaw, C.P., and Leaf, P.J. (2008). A multilevel study of predictors of student perceptions of school climate: The effect of classroom-level factors. Journal of Educational Psychology, 100(1), 96-104.
Kraag, G., Zeegers, M.P., Kok, G., Hosman, C., and Abu-Saad, H.H. (2006). School programs targeting stress management in children and adolescents: A meta-analysis. Journal of School Psychology, 44(6), 449-472.
Kutash, K., Duchnowski, A.J., and Lynn, N. (2006). School-based Mental Health: An Empirical Guide for Decision-makers. Louis de la Parte Florida Mental Health Institute, Department of Child and Family Studies, Research and Training Center for Children’s Mental Health. Tampa: University of South Florida,
Lanza, S.T., and Rhoades, B.L. (2013). Latent class analysis: An alternative perspective on subgroup analysis in prevention and treatment. Prevention Science, 14(2), 157-168.
Larimer, M.E., and Neighbors, C. (2003). Normative misperception and the impact of descriptive and injunctive norms on college student gambling. Psychology of Addictive Behaviors, 17(3), 235-243.
Leff, S.S., and Waasdorp, T.E. (2013). Effect of aggression and bullying on children and adolescents: Implications for prevention and intervention. Current Psychiatry Reports, 15(3), 1-10.
Lereya, S.T., Copeland, W.E., Costello, E.J., and Wolke, D. (2015). Adult mental health consequences of peer bullying and maltreatment in childhood: Two cohorts in two countries. The Lancet Psychiatry, 2(6), 524-531.
Lewis, T.J., and Sugai, G. (1999). Effective behavior support: A systems approach to proactive schoolwide management. Focus on Exceptional Children, 31(6), 1-24.
Limbos, M.A., Chan, L.S., Warf, C., Schneir, A., Iverson, E., Shekelle, P., and Kipke, M.D. (2007). Effectiveness of interventions to prevent youth violence: A systematic review. American Journal of Preventive Medicine, 33(1), 65-74.
Lindsley, O.R. (1992). Why aren’t effective teaching tools widely adopted? Journal of Applied Behavior Analysis, 25(1), 21-26.
Lochman, J.E., Wells, K.C., Qu, L., and Chen, L. (2013). Three-year follow-up of Coping Power intervention effects: Evidence of neighborhood moderation? Prevention Science, 14(4), 364-376.
Magalnick, H., and Mazyck, D. (2008). Role of the school nurse in providing school health services. Pediatrics, 121(5), 1052-1056.
Matjasko, J.L., Vivolo-Kantor, A.M., Massetti, G.M., Holland, K.M., Holt, M.K., and Cruz, J.D. (2012). A systematic meta-review of evaluations of youth violence prevention programs: Common and divergent findings from 25 years of meta-analyses and systematic reviews. Aggression and Violent Behavior, 17(6), 540-552.
McElearney, A., Adamson, G., Shevlin, M., and Bunting, B. (2013). Impact evaluation of a school-based counselling intervention in Northern Ireland: Is it effective for pupils who have been bullied? Child Care in Practice, 19(1), 4-22.
Menesini, E., Nocentini, A., and Palladino, B.E. (2012). Empowering students against bullying and cyberbullying: Evaluation of an Italian peer-led model. International Journal of Conflict and Violence, 6(2), 313-320.
Merrell, K.W., Gueldner, B.A., Ross, S.W., and Isava, D.M. (2008). How effective are school bullying intervention programs? A meta-analysis of intervention research. School Psychology Quarterly, 23(1), 26-42.
Meyer, N., and Lesch, E. (2000). An analysis of the limitations of a behavioural programme for bullying boys from a subeconomic environment. Southern African Journal of Child and Adolescent Mental Health, 12(1), 59-69.
Miles, P., Bruns, E., Osher, T., and Walker, J. (2006). The Wraparound Process User’s Guide: A Handbook for Families. National Wraparound Initiative Advisory Group, Research and Training Center on Family Support and Children’s Mental Health. Portland, OR: Portland State University.
Minton, S.J. (2014). Prejudice and effective anti-bullying intervention: Evidence from the bullying of “minorities.” Nordic Psychology, 66(2), 108-120.
Mishna, F., Khoury-Kassabri, M., Gadalla, T., and Daciuk, J. (2012). Risk factors for involvement in cyber bullying: Victims, bullies and bully–victims. Children and Youth Services Review, 34(1), 63-70.
Mytton, J.A., DiGuiseppi, C., Gough, D.A., Taylor, R.S., and Logan, S. (2002). School-based violence prevention programs: Systematic review of secondary prevention trials. Archives of Pediatrics and Adolescent Medicine, 156(8), 752-762.
Nansel, T.R., Overpeck, M.D., Haynie, D.L., Ruan, W.J., and Scheidt, P.C. (2003). Relationships between bullying and violence among U.S. youth. Archives of Pediatrics and Adolescent Medicine, 157(4), 348-353.
National Center for Health Statistics and National Center for Health Services Research. (2001). Health, United States. Public Health Service, Health Resources Administration, National Center for Health Statistics. Washington, DC: U.S. Department of Health, Education, and Welfare.
National Research Council and Institute of Medicine. (2009). Preventing Mental, Emotional, and Behavioral Disorders Among Young People: Progress and Possibilities. Committee on the Prevention of Mental Disorders and Substance Abuse Among Children, Youth, and Young Adults: Research Advances and Promising Interventions. M.E. O’Connell, T. Boat, and K.E. Warner, Editors. Board on Children, Youth, and Families, Division of Behavioral and Social Sciences and Education. Washington, DC: The National Academies Press.
Neighbors, C., Larimer, M.E., and Lewis, M.A. (2004). Targeting misperceptions of descriptive drinking norms: Efficacy of a computer-delivered personalized normative feedback intervention. Journal of Consulting and Clinical Psychology, 72(3), 434-447.
Nickel, M.K., Muehlbacher, M., Kaplan, P., and Krawczyk, J. (2006). Influence of family therapy on bullying behaviour, cortisol secretion, anger, and quality of life in bullying male adolescents: A randomized, prospective, controlled study. Canadian Journal of Psychiatry, 51(6), 355-362.
O’Brennan, L.M., Waasdorp, T.E., and Bradshaw, C.P. (2014). Strengthening bullying prevention through school staff connectedness. Journal of Educational Psychology, 106(3), 870-880.
Olweus, D. (1993). Bullying at School: What We Know and What We Can Do. Oxford, UK: Blackwell.
Olweus, D. (2005). A useful evaluation design, and effects of the Olweus Bullying Prevention Program. Psychology, Crime & Law, 11(4), 389-402.
Olweus, D., Limber, S., and Mihalic, S.F. (1999). Bullying Prevention Program: Blueprints for Violence Prevention. Blueprints for Violence Prevention Series, Center for the Study and Prevention of Violence, Institute of Behavioral Science, University of Colorado. Available: https://www.ncjrs.gov/pdffiles1/Digitization/174202NCJRS.pdf [June 2016].
Ortega-Ruiz, R., Del Rey, R., and Casas, J.A. (2012). Knowing, building and living together on Internet and social networks: The ConRed Cyberbullying Prevention Program. International Journal of Conflict and Violence, 6(2), 302-312.
Paluck, E.L., Sheperd, H., and Aronow, P.M. (2016). Changing climates of conflict: A social network experiment in 56 schools. Proceedings of the National Academy of Sciences of the United States of America 113(3), 566-571.
Palladino, E., Nocentini, A., and Menesini, E. (2016). Evidence-based intervention against bullying and cyberbullying: Evaluation of the NoTrap! Program through two independent trials. Aggressive Behavior, 42(2), 194-206.
Parr, M., Dagley, P.J., Pogrund, A., and MacDonell, L. (2012). Bullying: A Report from the Huntington Beach Human Relations Task Force. Available: http://www.ci.huntington-beach.ca.us/government/boards_commissions/pdf-files/2800-May-2012-Bullying-Report.pdf [Febuary 2016].
Pepler, D.J., Craig, W.M., and O’Connell, P., and Charach, A. (2004). Making a difference in bullying: Evaluation of a systemic school-based program in Canada. In P.K. Smith, D. Pepler and K. Rigby (Eds.), Bullying in Schools: How Successful Can Interventions Be? (pp. 125-140). Cambridge, UK: Cambridge University Press.
Petras, H., Kellam, S.G., Brown, C.H., Muthén, B.O., Ialongo, N.S., and Poduska, J.M. (2008). Developmental epidemiological courses leading to antisocial personality disorder and violent and criminal behavior: Effects by young adulthood of a universal preventive intervention in first-and second-grade classrooms. Drug and Alcohol Dependence, 95, S45-S59.
Pittet, I., Berchtold, A., Akre, C., Michaud, P.A., and Suris, J.C. (2009). Are adolescents with chronic conditions particularly at risk for bullying? Archives of Disease in Childhood, 95(9), 711-716.
Poduska, J.M., Kellam, S.G., Wang, W., Brown, C.H., Ialongo, N.S., and Toyinbo, P. (2008). Impact of the Good Behavior Game, a universal classroom-based behavior intervention, on young adult service use for problems with emotions, behavior, or drugs or alcohol. Drug and Alcohol Dependence, 95, S29-S44.
Polanin, J.R., Espelage, D.L., and Pigott, T.D. (2012). A meta-analysis of school-based bullying prevention programs’ effects on bystander intervention behavior. School Psychology Review, 41(1), 47-65.
Polanin, M., and Vera, E. (2013). Bullying prevention and social justice. Theory into Practice, 52(4), 303-310.
Poteat, V.P., Sinclair, K.O., DiGiovanni, C.D., Koenig, B.W., and Russell, S.T. (2013). Gay–straight alliances are associated with student health: A multischool comparison of LGBTQ and heterosexual youth. Journal of Research on Adolescence, 23(2), 319-330.
Poteat, V.P., Yoshikawa, H., Calzo, J.P., Gray, M.L., DiGiovanni, C.D., Lipkin, A., Mundy-Shephard, A., Perrotti, J., Scheer, J.R., and Shaw, M.P. (2015). Contextualizing gay-straight alliances: Student, advisor, and structural factors related to positive youth development among members. Child Development, 86(1), 176-193.
Richard, J.F., Schneider, B.H., and Mallet, P. (2012). Revisiting the whole-school approach to bullying: Really looking at the whole school. School Psychology International, 33(3), 263-284.
Riese, A., Gjelsvik, A., and Ranney, M.L. (2015). Extracurricular activities and bullying perpetration: Results from a nationally representative sample. Journal of School Health, 85(8), 544-551.
Rigby, K., and Slee, P. (2008). Interventions to reduce bullying. International Journal of Adolescent Medicine and Health, 20(2), 165-183.
Robbins, M., Szapocznik, J., and Pérez, G.A. (2007). Brief Strategic Family Therapy. In N. Kazantzia and L. L’Abate (Eds.), Handbook of Homework Assignments in Psychotherapy (pp. 133-149). New York: Springer.
Robbins, M.S., Bachrach, K., and Szapocznik, J. (2002). Bridging the research-practice gap in adolescent substance abuse treatment: The case of Brief Strategic Family Therapy. Journal of Substance Abuse Treatment, 23(2), 123-132.
Robers, S., Zhang, A., Morgan, R.E., Musu-Gillette, L. (2015). Indicators of School Crime and Safety: 2014 (NCES 2015-072/NCJ 248036). National Center for Education Statistics, U.S. Department of Education, and Bureau of Justice Statistics, Office of Justice Programs, U.S. Department of Justice. Washington, D.C: U.S. Government Publishing Office.
Robles-Piña, R.A., and Denham, M.A. (2012). School resource officers for bullying interventions: A mixed-methods analysis. Journal of School Violence, 11(1), 38-55.
Romer, D., Jamieson, P.E., and Jamieson, K.H. (2006). Are news reports of suicide contagious? A stringent test in six U.S. cities. Journal of Communication, 56(2), 253-270.
Ross, S.W., and Horner, R.H. (2009). Bullying prevention in positive behavior support. Journal of Applied Behavior Analysis, 42(4), 747-759.
Ryan, K.N., and Curwen, T. (2013). Cyber-victimized students: Incidence, impact, and intervention. SAGE Open, 3(4), 1-7.
Salmivalli, C. (2001). Peer-led intervention campaign against school bullying: Who considered it useful, who benefited? Educational Research, 43(3), 263-278.
Salmivalli, C. (2010). Bullying and the peer group: A review. Aggression and Violent Behavior, 15(2), 112-120.
Salmivalli, C. (2014). Participant roles in bullying: How can peer bystanders be utilized in interventions? Theory into Practice, 53(4), 286-292.
Salmivalli, C., Lagerspetz, K., Björkqvist, K., Österman, K., and Kaukiainen, A. (1996). Bullying as a group process: Participant roles and their relations to social status within the group. Aggressive Behavior, 22(1), 1-15.
Sanders, M.R., Markie-Dadds, C., Tully, L.A., and Bor, W. (2000). The Triple P—-Positive Parenting Program: A comparison of enhanced, standard, and self-directed behavioral family intervention for parents of children with early onset conduct problems. Journal of Consulting and Clinical Psychology, 68(4), 624-640.
Sapouna, M., Wolke, D., Vannini, N., Watson, S., Woods, S., Schneider, W., Enz, S., Hall, L., Paiva, A., and André, E. (2010). Virtual learning intervention to reduce bullying victimization in primary school: A controlled trial. Journal of Child Psychology and Psychiatry, 51(1), 104-112.
Sawyer, A.M., Borduin, C.M., and Dopp, A.R. (2015). Long-term effects of prevention and treatment on youth antisocial behavior: A meta-analysis. Clinical Psychology Review, 42, 130-144.
Schaeffer, C.M., and Borduin, C.M. (2005). Long-term follow-up to a randomized clinical trial of multisystemic therapy with serious and violent juvenile offenders. Journal of Consulting and Clinical Psychology, 73(3), 445-453.
Sexton, T.L., and Alexander, J.F. (2000). Functional family therapy. Juvenile Justice Bulletin, December. Available: https://www.ncjrs.gov/pdffiles1/ojjdp/184743.pdf [June 2016].
Shields, A., and Cicchetti, D. (2001). Parental maltreatment and emotion dysregulation as risk factors for bullying and victimization in middle childhood. Journal of Clinical Child Psychology, 30(3), 349-363.
Shonkoff, J.P., Garner, A.S., Siegel, B.S., Dobbins, M.I., Earls, M.F., McGuinn, L., Pascoe, J., and Wood, D.L. (2012). The lifelong effects of early childhood adversity and toxic stress. Pediatrics, 129(1), e232-e246.
Smith, J.D., Schneider, B.H., Smith, P.K., and Ananiadou, K. (2004). The effectiveness of whole-school antibullying programs: A synthesis of evaluation research. School Psychology Review, 33(4), 547-560.
Storch, E.A., Heidgerken, A.D., Geffken, G.R., Lewin, A.B., Ohleyer, V., Freddo, M., and Silverstein, J.H. (2006). Bullying, regimen self-management, and metabolic control in youth with Type I diabetes. The Journal of Pediatrics, 148(6), 784-787.
Stuart-Cassel, V., Bell, A., and Springer, J.F. (2011). Analysis of State Bullying Laws and Policies. Washington, DC: Office of Planning, Evaluation and Policy Development, U.S. Department of Education.
Sugai, G., and Horner, R.R. (2006). A promising approach for expanding and sustaining school-wide positive behavior support. School Psychology Review, 35(2), 245-259.
Sugai, G., Horner, R.H., and Gresham, F.M. (2002). Behaviorally effective school environments. In M.R. Shinn, H.M, Walker, and G. Stoner (Eds.), Interventions for Academic and Behavior Problems II: Preventive and Remedial Approaches. Washington, DC: National Association of School Psychologists.
Swearer, S., Espelage, D., Koenig, B., Berry, B., Collins, A., and Lembeck, P. (2012). A social-ecological model of bullying prevention and intervention in early adolescence. In S.R. Jimberson, A.B. Nickerson, M.J. Mayer, and M.J. Furlong (Eds.), Handbook of School Violence and School Safety: International Research and Practice (pp. 333-355). New York: Routledge.
Swearer, S.M., Espelage, D.L., Vaillancourt, T., and Hymel, S. (2010). What can be done about school bullying?: Linking research to educational practice. Educational Researcher, 39(1), 38-47.
Swearer, S.M., Wang, C., Collins, A., Strawhun, J., and Fluke, S. (2014). Bullying: A school mental health perspective. In M.D. Weist, N.A. Lever, C.P. Bradshaw, and J.S. Owens (Eds.), Handbook of School Mental Health: Research, Training, Practice and Policy (pp. 341-354). New York: Springer.
Szapocznik, J., and Williams, R.A. (2000). Brief Strategic Family Therapy: Twenty-five years of interplay among theory, research and practice in adolescent behavior problems and drug abuse. Clinical Child and Family Psychology Review, 3(2), 117-134.
Tierney, T., and Dowd, R. (2000). The use of social skills groups to support girls with emotional difficulties in secondary schools. Support for Learning, 15(2), 82-85.
Ttofi, M.M., and Farrington, D.P. (2009). What works in preventing bullying: Effective elements of anti-bullying programmes. Journal of Aggression, Conflict and Peace Research, 1(1), 13-24.
Ttofi, M.M., and Farrington, D.P. (2011). Effectiveness of school-based programs to reduce bullying: A systematic and meta-analytic review. Journal of Experimental Criminology, 7(1), 27-56.
Ttofi, M.M., and Farrington, D.P. (2012). Risk and protective factors, longitudinal research, and bullying prevention. New Directions for Youth Development, 2012(133), 85-98.
Ttofi, M.M., Eisner, M., and Bradshaw, C.P. (2014). Bullying prevention: Assessing existing meta-evaluations. In G. Bruinsma and D. Weisburd (Eds.), Encyclopedia of Criminology and Criminal Justice (pp. 231-242). New York: Springer.
Twyman, K.A., Saylor, C.F., Saia, D., Macias, M.M., Taylor, L.A., and Spratt, E. (2010). Bullying and ostracism experiences in children with special health care needs. Journal of Developmental & Behavioral Pediatrics, 31(1), 1-8.
U.S. Census Bureau. (2014). Nearly 6 out of 10 Children Participate in Extracurricular Activities, Census Bureau Reports (U.S. Census Bureau press release). Available: https://www.census.gov/newsroom/press-releases/2014/cb14-224.html [December 2015].
U.S. Department of Education. (2015). 21st Century Community Learning Centers—Resources. Available: http://www2.ed.gov/programs/21stcclc/resources.html [December 2015].
U.S. Department of Health and Human Services. (2015). Bullying Prevention Training Center. Available: http://www.stopbullying.gov/prevention/training-center/ [December 2015].
van der Stouwe, T., Asscher, J.J., Stams, G.J.J., Deković, M., and van der Laan, P.H. (2014). The effectiveness of Multisystemic Therapy (MST): A meta-analysis. Clinical Psychology Review, 34(6), 468-481.
Vannini, N., Enz, S., Sapouna, M., Wolke, D., Watson, S., Woods, S., Dautenhahn, K., Hall, L., Paiva, A., and André, E. (2011). “FearNot!”: A computer-based anti-bullying-programme designed to foster peer intervention. European Journal of Psychology of Education, 26(1), 21-44.
Veenstra, R., Lindenberg, S., Huitsing, G., Sainio, M., and Salmivalli, C. (2014). The role of teachers in bullying: The relation between antibullying attitudes, efficacy, and efforts to reduce bullying. Journal of Educational Psychology, 106(4), 1135-1143.
Vessey, J.A., DiFazio, R.L., and Strout, T.D. (2013). Youth bullying: A review of the science and call to action. Nursing Outlook, 61(5), 337-345.
Vreeman, R.C., and Carroll, A.E. (2007). A systematic review of school-based interventions to prevent bullying. Archives of Pediatrics and Adolescent Medicine, 161(1), 78-88.
Waasdorp, T.E., and Bradshaw, C.P. (2011). Examining student responses to frequent bullying: A latent class approach. Journal of Educational Psychology, 103(2), 336-352.
Waasdorp, T.E., and Bradshaw, C.P. (2015). The overlap between cyberbullying and traditional bullying. Journal of Adolescent Health, 56(5), 483-488. Available: http://dx.doi.org/10.1016/j.jadohealth.2014.12.002 [November 2015].
Waasdorp, T.E., Bradshaw, C.P., and Duong, J. (2011). The link between parents’ perceptions of the school and their responses to school bullying: Variation by child characteristics and the forms of victimization. Journal of Educational Psychology, 103(2), 324-335.
Waasdorp, T.E., Bradshaw, C.P., and Leaf, P.J. (2012). The impact of schoolwide positive behavioral interventions and supports on bullying and peer rejection: A randomized controlled effectiveness trial. Archives of Pediatrics and Adolescent Medicine, 166(2), 149-156.
Wakefield, M.A., Loken, B., and Hornik, R.C. (2010). Use of mass media campaigns to change health behaviour. The Lancet, 376(9748), 1261-1271.
Walker, H.M., Horner, R.H., Sugai, G., Bullis, M., Sprague, J.R., Bricker, D., and Kaufman, M.J. (1996). Integrated approaches to preventing antisocial behavior patterns among school-age children and youth. Journal of Emotional and Behavioral Disorders, 4(4), 194-209.
Wang, J., Iannotti, R.J., and Nansel, T.R. (2009). School bullying among adolescents in the United States: Physical, verbal, relational, and cyber. Journal of Adolescent Health, 45(4), 368-375.
Webster-Stratton, C. (1999). How to Promote Children’s Social and Emotional Competence. London: Paul Chapman.
Webster-Stratton, C., Jamila Reid, M., and Stoolmiller, M. (2008). Preventing conduct problems and improving school readiness: Evaluation of the Incredible Years teacher and child training programs in high-risk schools. Journal of Child Psychology and Psychiatry, 49(5), 471-488.
Weisz, J.R., Sandler, I.N., Durlak, J.A., and Anton, B.S. (2005). Promoting and protecting youth mental health through evidence-based prevention and treatment. American Psychologist, 60(6), 628-648.
Wilcox, H.C., Kellam, S.G., Brown, C.H., Poduska, J.M., Ialongo, N.S., Wang, W., and Anthony, J.C. (2008). The impact of two universal randomized first-and second-grade classroom interventions on young adult suicide ideation and attempts. Drug and Alcohol Dependence, 95, S60-S73.
Wilson, S.J., and Lipsey, M.W. (2007). School-based interventions for aggressive and disruptive behavior: Update of a meta-analysis. American Journal of Preventive Medicine, 33(2), S130-S143.
Wolke, D., and Lereya, S.T. (2015). Long-term effects of bullying. Archives of Disease in Childhood, 100(9), 879-885.
Ybarra, M.L., and Mitchell, K.J. (2004). Online aggressor/targets, aggressors, and targets: A comparison of associated youth characteristics. Journal of Child Psychology and Psychiatry, 45(7), 1308-1316.
Yeager, D.S., Fong, C.J., Lee, H.Y., and Espelage, D.L. (2015). Declines in efficacy of antibullying programs among older adolescents: Theory and a three-level meta-analysis. Journal of Applied Developmental Psychology, 37, 36-51.










































































