
8
Community Engagement and Patient Advocacy
The community-based organizations are valued. I would consider them like the gatekeepers to the sickle cell disease community. They definitely have their finger on the pulse of the community.
—Shauna W. (Open Session Panelist)
continued
HISTORICAL PERSPECTIVE
Individuals living with sickle cell disease (SCD) and sickle cell trait (SCT) often experience racism, stigma, and implicit bias within and outside the health care system. SCD-specific community-based organizations (CBOs) have been and continue to be important in mitigating these experiences and therefore have a critical role in any strategic initiative to improve care and services for this population.
As discussed in earlier chapters of this report, individuals living with SCD and SCT were and continue to be socially stigmatized and neglected in the health care system because of the lack of general understanding of the disease and its consequences. This current state is best understood in the context of the historical experiences that have shaped advocacy and community engagement. In response to social activism in the 1960s regarding the poor health of African Americans, an activism that was catalyzed by the Black Panther Party, President Nixon told Congress in a 1971 speech that “a second targeted disease for concentrated research should be sickle cell anemia.… It is a sad and shameful fact that the causes of this disease have been largely neglected throughout our history. We cannot rewrite this record of neglect, but we can reverse it” (Gold, 2017).
In conjunction with this increased attention to SCD, 12 states and the District of Columbia enacted mandatory sickle cell screening laws for African Americans. Most of these laws equated SCT with SCD. These laws led to stigmatizing people with carrier status, resulting in such things as denial of health and life insurance, poorer employment opportunities, and rejection from the U.S. Air Force Academy (Markel, 1992). In 1972, the call for a special effort to address SCD led to the passage of the National Sickle Cell Anemia Control Act (Public Law 92-294) (Manley, 1984). One important aspect of the act is that it ended mandatory genetic testing for SCD. The act made testing voluntary; provided $6 million dollars toward research into and treatment of SCD; and authorized education, information, screening, testing, genetic counseling, research, and treatment programs to improve understanding (Manley, 1984).
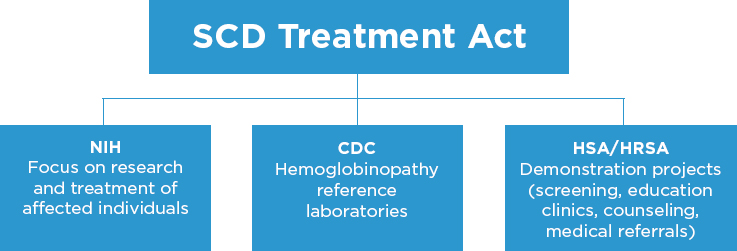
NOTE: CDC = Centers for Disease Control and Prevention; HRSA = Health Resources and Services Administration; HSA = Health Services Administration; NIH = National Institutes of Health; SCD = sickle cell disease.
The decade after the National Sickle Cell Control Act was passed featured increased awareness of and efforts to educate the public about SCD and SCT and to develop and evaluate new therapies. In the early 1970s the federal efforts focused on SCD and SCT involved three major agencies (see Figure 8-1): the National Institutes of Health (NIH); the Health Services Administration (HSA), later renamed the Health Resources and Services Administration (HRSA), and the Centers for Disease Control and Prevention (CDC).
NIH focused on research and treatment. HSA and HRSA translated this work and established demonstration projects for screening, education clinics for counseling, and medical referral for those diagnosed with SCD, specifically through the Maternal and Child Health Bureau (MCHB). CDC focused on developing hemoglobinopathy laboratories and training programs to provide proficiency testing and also to serve as reference laboratories. Under the administration of NIH, the comprehensive SCD treatment centers were established, with the goal of reducing morbidity and mortality (Manley, 1984).
The HSA sickle cell clinics were the nexus of connectivity with the community and offered genetic counseling and awareness education, referring those identified as having SCD to the NIH comprehensive centers. The centers were supported by an interagency transfer of funds from NIH that began in 1972 with $1.9 million, increasing to $3.4 million in 1974. The number of centers rapidly expanded from 19 in 1972 to 26 in 1975, with the majority located in the southeast United States, where there was a dense population of African Americans. This initiative established a protocol for education and counseling for SCD through the sickle cell clinics. In 1976 the Genetic Disease Act was passed, with a mandate
to provide genetic services for all genetic conditions, including SCD, affording MCHB a platform to establish structures for serving individuals with SCD. By 1982 a reported 1.6 million clients had been educated and 860,000 clients screened. The concept of the SCD CBO was an integral part of the original design of SCD services introduced by the National Sickle Cell Control Act.
Unfortunately, federal funding appropriation was far less than what was needed to provide services for all genetic diseases. In addition, it was delegated to states to incorporate sickle cell into their genetics service delivery networks and MCHB programs. Further restructuring of the funding mechanisms for genetic diseases inherently modified the clinic structure and functions and the overall delivery of SCD services; this dismantled the robust infrastructure established by the federal mandate, giving rise to a fragmented SCD care delivery system in which individual states controlled screening and follow-up with other services, such as data collection, research, and clinical services, split among various federal agencies.
Despite the National Sickle Cell Control Act, discrimination borne out of misinformation and a lack of knowledge about persons with SCD and SCT did not end. National funding for SCD was tied to congressional appropriations, which resulted in a “push–pull” on research funding between SCD and other disease groups. Failure to distinguish SCT, the carrier state affecting millions of Americans, from SCD led to an incorrect labeling of SCT as SCD and resulted in needless fears and discrimination for many individuals. The general public and some physicians reinforced this medical mismanagement and bias, resulting in individuals with SCT being denied education, insurance, and employment opportunities (Scott, 1981). Moreover, the poorly conceived design and inadequate resources of the clinics may have contributed to improper and inadequate testing procedures, incorrect interpretation of test results, and misinformed genetic counseling. There was little supervision of the interpretation of genetic testing results by trained medical professionals, and counseling services were inconsistent, causing undue harm from miscommunication and misinterpretation of results (Scott, 1981).
To avoid a repeat of the negative consequences associated with the National Sickle Cell Control Act, any national strategy that addresses identified priorities for SCD and SCT requires critical information and feedback from the SCD community. However, the work of the advocates/advocacy groups and CBOs (formerly housed within the clinics) is hampered by important obstacles discussed in this chapter, which will need to be addressed if the full potential of the community is to be harnessed and the relevant stakeholders to be engaged in advancing care, outcomes, and resources for the SCD population. Most importantly, there is a need to develop a structured and scalable value framework for the contribution that CBOs provide
toward improving care outcomes that will allow adequate infrastructure and financial support for their continued existence.
SICKLE CELL COMMUNITY-BASED ORGANIZATIONS AND PATIENT ADVOCACY GROUPS
SCD is the largest of the rare genetic diseases, yet it lacks the coordinated efforts and unified patient voice needed to make a difference. The current landscape of SCD patient organizations is complex. There are multiple stakeholders operating at various levels (federal, state, and local), and they may conduct brick-and-mortar or virtual (not bound by geography) activities or a combination of both. There are community- and health system–based support groups for individuals living with SCD and their families, and there are smaller groups established by individuals affected by SCD and their families. Patient advocates or groups may influence policy, programs, resource allocation, and messaging to relevant stakeholders and the general public about the interests, needs, and well-being of the SCD population.
SCD CBOs encompass a wide variety of entities, from independent individual advocates to small local groups focused on sickle cell awareness and education to large national groups, including organizations delivering enabling services. These organizations are also involved in community engagement, which is the “inclusion of local health system users and community resources in all aspects of design, planning, governance, and delivery of health care services” (PHCPI, 2018). Patient advocates, advocacy groups, and CBOs may liaise between the SCD population and the care delivery system; as discussed later in this chapter, most diseases, especially rare and inheritable diseases, have benefited from the work of strong patient organizations. CBOs and advocacy groups carry out sets of activities based on their organizational structures, but the lack of coordination among these groups results in a duplication of activities, primarily because the various organizations typically operate independently. This has limited their overall effectiveness and served as an impediment to having a far-reaching impact.
National efforts that encompass the interests of all CBOs and advocacy groups regardless of size, infrastructure, mission, and capacity are challenging, particularly in SCD, where all entities are under-resourced. The CDC National Resource Directory (CDC, 2019b) identifies two SCD resources working at the national level to advance awareness, care, and outcomes: the Sickle Cell Disease Association of America (SCDAA) and the Sickle Cell Community Consortium (SCCC). These two groups are vastly different in focus, structure, and scope.
There are several CBOs and advocacy groups operating at the state and local levels to advocate for and support the SCD community. Some of these organizations may be members and affiliates of SCDAA or other national
organizations discussed later in this chapter, but they still operate independently. Appendix K lists CBOs and advocacy resource groups related to SCD, identified using publicly available information and online sources, including all state-level chapters of SCDAA. However, this list is not fully inclusive; it is only meant to provide an overview of SCD patient organizations by state. There is no available comprehensive listing or registry of SCD CBOs or advocacy groups, nor is there a standardized classification of precisely which services each offers. Thus, there is an opportunity to create a comprehensive cataloguing of CBOs and community resources available for the SCD population and to develop a formal characterization and classification of the various services that each offers.
Services Offered by SCD Community-Based Organizations
SCD CBOs provide a myriad of services beyond awareness about SCD and SCT and advocacy that support and complement health care for children and adults; these include education, counseling, care coordination, and enabling services (see Table 8-1). The influence and overall impact of the SCD CBOs remains invisible in the scientific literature because community participation, engagement, and support are not typically measured with the current scientific publications. CBOs, by dint of their defined scope and sphere, are embedded in their communities, understand the dynamics and needs of these communities, and can tailor their offerings accordingly.
The activities in Table 8-1 can be categorized into three key categories of functions discussed in the next sections: providing public education and awareness, providing enabling services to the SCD population, and bridging the SCD population and the scientific and clinical community.
Providing Public Education and Awareness
Public awareness and information serve to demystify a health condition. This is especially needed for SCD/SCT, as alluded to in preceding chapters. Public awareness and understanding of the disease are limited, which places the burden on individuals to educate those in their milieu (e.g., health care, schools, places of employment, clinics). It is also important to ensure that public information about SCT is factually accurate and that misinformation is promptly debunked so as to avoid a repeat of the 1970s situation when SCT was confounded with SCD, resulting in stigmatizing people with carrier status. CBOs and other patient advocacy groups assume the collective voice of individuals with SCD and SCT and play a pivotal role in educating the public and key stakeholders, especially legislators. These groups require access to appropriate and accurate information and education and the necessary counseling and health education skills to ensure that
| Service | Description of Activities |
|---|---|
| SCD and SCT education |
|
| Genetic counseling services |
|
| Psychosocial support |
|
| Camps |
|
| Care coordination |
|
| Case finding and referral to care |
|
| Enabling services |
|
| Clinical trial education and recruitment |
|
| Transition assistance |
|
NOTE: CBO = community-based organization; SCD = sickle cell disease; SCDAA = Sickle Cell Disease Association of America; SCT = sickle cell trait.
they communicate accurate and up-to-date information about SCD and SCT to broad audiences. The optimal purpose of such public awareness campaigns is to share accurate information with all.
In a recent campaign about self-management education awareness, CDC demonstrated that the important components of public awareness efforts include having a clear, concise, and simple message; engaging all relevant partners and stakeholders; and providing access to additional (vetted) readily available informational resources in various accessible formats for individuals and stakeholders. A similar structured process to communicate awareness messages for use by all SCD CBOs and advocacy groups would result in less misinformation and fewer potentially conflicting messages. One way to ensure consistency and accuracy in messaging would be to develop a centralized toolkit that all advocacy and CBO groups could use to provide evidence-based, culturally appropriate information at the appropriate literacy level in their awareness campaigns. The federal government, in collaboration with relevant organizations, could develop such a toolkit.
Providing Enabling Services to the SCD Population
CBOs and patient advocacy groups are best positioned to provide certain enabling services, including social and peer support, hospital visitation, and recreational and social activities, to address the isolation and need for community that individuals with SCD have expressed. CBOs may also provide services tailored to mitigating various nonmedical social needs, such as transportation to and from medical appointments; assistance with basic needs, such as housing, utilities, food, child care, and tutoring; and linkage to other community resources, such as vocational training and legal clinics to help with disability insurance. Many of these services are provided by community health workers (CHWs) who work within CBOs or medical centers.
Many CBOs provide an annual SCD camp, which is an important enabling service. For children with chronic disease, the summer camp experience can support education and quality-of-life (QOL) benefits through opportunities for peer modeling, disease education, and reduced isolation. The committee heard from young adult panelists in the open session of the fourth meeting that an SCD camp is a valuable service that not only addresses the significant isolation that individuals experience but also serves as a pipeline for SCD advocates who attended camp as children, returned as camp counselors, and continue on to find their niche as advocates in the SCD community.
There are several categories of camp experiences for children and young adults with SCD. Many involve 1- to 2-week experiences for children, with
or without their siblings. The camps are staffed by the sponsoring CBO and volunteers. There are also national camps that provide experiences for children with chronic illnesses in general. Many of these camps offer “sickle cell only” weeks on their properties supported by their regular camp staff and have medical teams on site that are familiar with the care of children and adults with SCD. Local health care systems work alongside CBOs locally to ensure that when campers have pain or fever, physicians and nurses are on site to provide care and to aid in transport to nearby health centers (Narcisse et al., 2018). Some providers use camp as an opportunity to strengthen the provider–patient relationship (DiDomizio and Gillard, 2018). Parents and caregivers are reassured and comforted when their local medical teams or others familiar with SCD are on staff. This provides opportunities for these children whose families might have limited their camp experiences otherwise. Expenses and charges for camp participation are supplemented or fully covered by philanthropy or grant funding. Finally, providing counselor-in-training and counselor positions for, respectively, teens and adults with SCD offers informal peer-mentoring and patient support systems.
Although sickle cell camps have been in existence for more than four decades, very little has been published on their key elements or on how the experience affects the lives of individuals living with SCD. The benefit of camps for children with chronic disease has been well demonstrated for inflammatory bowel disease (Salazar and Heyman, 2014; Shepanski et al., 2005), cancer (Wu et al., 2016), burns (Bakker et al., 2011), and pediatric diabetes (Bultas et al., 2016). Generally, camp experiences increase self-esteem, as participants learn that there are other children with SCD who may share similar problems. Campers enjoy the opportunity to play, participate in sports, swim, and live with other children with SCD without being forced to think about their illness. Some camps offer only recreational activities, while others provide opportunities to learn disease self-management, increase sickle cell knowledge, prepare for transition from pediatric to adult care, or learn life skills needed to get ready for college and vocations.
Narcisse et al. (2018) published on summer camps for SCD, highlighting the importance of appropriate staff training in adapting the camp schedule, activities, and environment to minimize the potential for exacerbating a vaso-occlusive episode (VOE). For example, camps can arrange for temperature control, access to water for liberal hydration, and schedules that allow for frequent breaks in order to prevent overexertion, which can trigger a VOE. The authors also recommend developing and disseminating standardized manuals to guide the operational structure and functions of an SCD-specific camp, including staff training, recruiting young adults with SCD as counselors, the appropriate medical team infrastructure based
on camper census, and standardization of suitable educational material and resources. It is imperative that research on the care needs of the SCD population, adolescent transition, and various QOL metrics, such as self-management, coping, and isolation, be conducted to guide resources offered at SCD camps.
Client engagement across the life span is difficult for any CBO serving a community with a chronic inherited condition. Camp may be the first time that a child with SCD has an experience involving the local CBO. This experience helps the CBO develop a relationship with the child before the transition to young adulthood. Relationships formed at camp can often be a source of support when a youth with SCD is hospitalized or struggling to keep up in school. These positive camp experiences cultivate participation in tutoring, reunions, seasonal parties, and other events.
Serving as a Bridge Between the SCD Population and the Scientific and Clinical Community
The final and key role of CBOs and patient advocacy groups is to connect individuals with SCD and SCT to the health care system. This function begins with newborn screening (NBS), for which some states partner with CBOs and patient advocacy groups to follow up with families of newborns with positive SCD results and link them with needed care. Although the committee was unable to find existing models for joint training, having CBO staff and medical practitioners participate together in training on how to work collaboratively would only enhance the relationship between the two.
CBOs also provide education about SCD and SCT to individuals and to the community to help with clinical and reproductive decision making. CBOs may partner with researchers at academic medical centers or private pharmaceutical manufacturers to disseminate information about clinical trials and recruit participants. This a crucial role for CBOs, especially in light of the historical injustices that African Americans have suffered in participating in investigational clinical research, which has fostered deep mistrust between the community and the health care system and has historically contributed to an unwillingness to participate in clinical trials.
Some CBOs offer services to aid young adults transitioning from pediatric to adult care by assessing transition readiness and providing education. Some organizations may even accompany young adults to their first adult clinical visit. CBOs also provide care coordination and case referral services. As discussed in Chapters 4, 5, and 6, the complexities of SCD and its associated complications necessitate care from a multidisciplinary
team, resulting in a situation that may be overwhelming for individuals and their families to navigate on their own. CBOs can assist people in finding a medical home that supports their whole-person needs (see Chapter 5) and with scheduling and coordinating services among multiple medical providers. When liaising between the SCD population and the health care system, CBOs often rely on CHWs, as other staff members may not be as facile at navigating the health care system. The CHW’s role is discussed in the next section.
The liaison role of the CBO and SCD advocacy groups should never be considered unilateral. While the focus is on supporting access to care for the individuals affected, historically CBOs have always been in a position of “supporter,” with no quid pro quo benefit. CBOs are often not included in scientific publications, even though they provide researchers with invaluable help in both developing strong grant applications and securing access to affected individuals. Their role as a liaison to the health care system and to research efforts is generally invisible. Without equal visibility as part of the research team in scientific publications, CBOs are relegated to the acknowledgment section of manuscripts and remain undervalued. While CBOs may lack the infrastructure to produce scientific literature, they are strong cultural brokers within the SCD community and are necessary for most scientific research advances. True partnership with the medical community will require redefining roles and their ascribed values, with clear guidelines for infrastructure and capacity building within CBOs to support their key function as a bridge between the SCD community and the health care system.
Community Health Workers
CHWs are also known as “outreach workers,” promotores/as de salud, “community health representatives,” and “patient navigators” (Rosenthal et al., 2010). Clinician scientists and several SCD CBOs across the country recently coproduced a publication that described the role of nonclinical CHWs in SCD care (Hsu et al., 2016). The authors cited the high socioeconomic and health burden of SCD as a public health concern and suggested that public health approaches might be able to mitigate the socio-ecological barriers that result in poor outcomes (which CHWs can address). Because care delivery for SCD, as with most chronic conditions, is complicated by disparities in health care access, delivery, services, and cultural provider–patient mismatches, the authors propose using CHWs to support case management, social support, and health system navigation (Hsu et al., 2016). CHWs would address multiple barriers faced in accessing the health care system and serve seven core roles in improving patients’ health, as detailed in Figure 8-2 (Hsu et al., 2016).
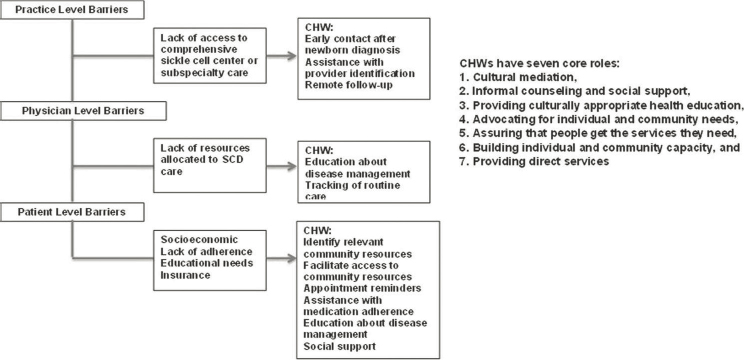
NOTE: CHW = community health worker; SCD = sickle cell disease.
SOURCE: Hsu et al., 2016.
There is evidence from the literature indicating that it may be effective to use CHWs to support and manage care for individuals with other chronic conditions, but there is very limited evidence for the SCD population (Otero-Sabogal et al., 2010; Rhodes et al., 2007; Rosenthal et al., 2010).
Examples of Community-Based Organizations and Patient Advocacy Groups and Services Provided
The capabilities and activities at CBOs and patient advocacy groups vary greatly. This section provides an overview of select CBOs and groups that are recognized for their active programming and patient advocacy efforts in the SCD population. Because there is little research and few publications on the contributions of such CBOs, the groups described here were identified through open session speaker remarks, information provided to the committee and National Academies team, and discussions with relevant stakeholders. Information on the groups’ activities was drawn from the public information on their websites.
Sickle Cell Disease Association of America
SCDAA was founded in 1971 as the National Association for Sickle Cell Disease (it updated its name in 1994). The association’s mission is “to advocate for people affected by sickle cell conditions and empower CBOs to maximize QOL and raise public consciousness while advancing the search
for a universal cure” (SCDAA, 2019). SCDAA has a network of state and local affiliated member organizations that are independent CBOs, which it works with to advance its mission (see Appendix K).
SCDAA supports a number of programs, including the CHW training program, a leadership academy that provides leadership skills, organizational effectiveness, and technical support for member CBOs, and also the National Sickle Cell Advocacy Network, which educates and empowers patients, families, caregivers, clinicians, stakeholders, and experts who are themselves affected by the disease or who want to advocate, educate, and help people living with SCD. The organization hosts an annual convention, which has been running for more than four decades and offers a platform for collaboration for more than 300 attendees (CBO member organizations, individuals living with SCD and SCT, health care professionals, and researchers) to share and learn from each other. SCDAA also developed Get Connected, the first patient-powered registry.
SCDAA is funded by a variety of sources, including federal grants, such as HRSA’s Sickle Cell Disease Newborn Screening Follow-Up Program, which provides the resources for the organization to work with CBOs across the country in order to improve access to quality care for the SCD population, and it has strategic partnerships with various other philanthropic organizations. A major SCDAA initiative is the organization’s national advocacy day, where the community works strategically on legislation that will foster improved research and access to care.
Sickle Cell Disease Foundation of California
The Sickle Cell Disease Foundation of California (SCDFC), founded in 1957, was the first social service nonprofit founded to focus on the needs of the SCD population (Sickle Cell Disease Foundation, n.d.). Perhaps because of its longevity, the SCDFC offers a strong model of successful patient advocacy at the state level. SCDFC works collaboratively with the Center for Inherited Blood Disorders (CIBD), a safety net clinic in southern California that provides health care services for individuals with blood disorders. SCDFC and CIBD successfully advocated for adding $15 million to the state budget specifically to establish comprehensive sickle cell centers. Using data from their involvement in the CDC Sickle Cell Disease Data Project (CDC, 2019a), SCDFC spearheaded the advocacy efforts. It also led efforts by participating in the Pacific Regional Sickle Cell Collaborative, one of five regional grantees funded by HRSA as part of the U.S. Sickle Cell Disease Treatment Demonstration Program (SCDTDP), to expand access to health care through the establishment of the MLK Jr. Outpatient Center for Adults with SCD (Sickle Cell Disease Foundation, n.d.). SCDFC provides support services, patient education, and public awareness and fundraising activities;
it works according to an established, highly effective model that can offer insights for other patient advocacy groups.
Sickle Cell Foundation of Georgia
Camp New Hope really keeps a lot of kids together;
it keeps them feeling as though there is family, a community for us, that we all have something.
—Gregory G. (Open Session Panelist)
Since 1971 the Sickle Cell Foundation of Georgia (SCFGA) has served individuals with SCD and SCT in a variety of ways. In 2018, SCFGA provided services to 2,067 individuals in 64 counties across the state (SCFGA, 2018), including care coordination through the use of CHWs, assistance with applying to federal programs, testing and counseling to individuals with SCT, support groups, health fairs, and awareness events targeting the broader community. The Sickle Cell Road Race/Walk at Welcome All Park in Atlanta has been an annual awareness and fundraising event since 1979. SCFGA has a mobile trait testing unit, first donated by baseball legend Hank Aaron in 1973, which serves the entire state, providing access to trait testing and genetic counseling to rural areas.
Part of SCFGA’s mission is to provide education, awareness, and support to health care providers of all categories (physicians, advanced practice providers, nurses, residents, and medical students) through its partnerships with Emory University, Children’s Healthcare of Atlanta, and the Morehouse School of Medicine. It has developed a robust pediatric-to-adult transition support services program, working collaboratively with the Children’s Healthcare of Atlanta hospital and Grady Hospital SCD program to facilitate the education and engagement of young adults who are transitioning into adult care.
This initiative has been expanded to include support for youth beyond the transition age, whom it has mentored and trained to support its mission and objectives, including its role as a co-investigator on the Patient-Centered Outcomes Research Institute–funded transition study. It recently launched an initiative to build capacity among non-specialty providers to treat individuals with SCD in Georgia using a structured continuing medical education webinar and in-person curriculum and by broadly disseminating the American Society of Hematology (ASH) pocket guides for SCD clinical practice and various informational sheets about SCD therapies, such as hydroxyurea (HU) and Endari. In 2015 it established a CHW program funded through the HRSA/SCDAA NBS program to provide care coordination support to help link individuals with primary care medical homes.
It built partnerships with federally qualified health centers located in communities with the largest access to care gaps across 75 counties in Georgia.
For more than 40 years SCFGA has hosted a camp for children with SCD. The first day camp was sponsored in 1973, and the day camps later became retreats and (beginning in 1990) a week-long away camp. Camp New Hope, which patient speakers referenced as a source of support at the committee’s open session meeting, is staffed by volunteers, most of whom are living with SCD and attended the camp in the past. In 2018 the 1-week camp hosted 114 participating youth. In addition to relying on volunteers as camp counselors, the camp also ran a 24-hour infirmary staffed by 25 volunteers—12 physicians, 12 nurses, and 1 social worker (SCFGA, 2018). SCFGA also organizes charity events to promote public awareness and education and to advocate for legislation.
The Children’s Sickle Cell Foundation of Pittsburgh
The Children’s Sickle Cell Foundation launched a legislative agenda with an Advocacy Luncheon in 2009. Through the Pennsylvania Sickle Cell Provider’s Network (PASCPN), five CBOs work with four hospitals on issues directly affecting the sickle cell population across the state. PASCPN coordinates efforts to educate lawmakers during the Pennsylvania Supports Sickle Cell Disease Advocacy Day. Each year approximately 350 attendees wearing bright red shirts that read “PA Supports SCD” flock to the Pennsylvania State Capitol. Planning the advocacy day takes several months, and a core team consisting of a few representatives of the network works to reach consensus on the legislative priorities, talking points, program agenda, and logistics.
The Pennsylvania Legislative Black Caucus is an engaged partner and secures the venue for the morning press conference, lunch, and afternoon roundtable discussion with its key members. Each CBO arranges visits to important legislators and those representing its home district around the program schedule. Physicians, CBO leaders, individuals living with SCD, and parents and other family members meet with legislators or their staffers to speak directly from the talking points on their unique perspectives. Each meeting lasts about 15 minutes and usually ends with a photograph of the group and legislator.
One critical aspect of this legislative advocacy effort is to be intentional about including a follow-up plan. The legislative office provides a card with a follow-up contact, and it is important to reach out within a week or two to clarify any points or to simply offer thanks for their time and support.
In 2011 PASCPN responded to the proposed budget collapse of the sickle cell line item into a broader category line item, which would have resulted in removing dedicated funds for SCD. This issue was added to the legislative priorities that year, and as a result of educating both Democrat and Republican leaders the line item (and dedicated funding) was preserved.
This galvanized PASCPN, which continues to be successful in reaching and educating lawmakers and receiving support on issues of HU education and, most currently, addressing the effects of the opioid crisis on those in the state with SCD. Models like this help develop best practices that should be shared throughout the nation to help other states address these issues.
Sickle Cell Disease Association of Illinois
The Sickle Cell Disease Association of Illinois (SCDAI) was founded in 1971. SCDAI details a list of milestones that the organization has accomplished, including a grant awarded by HRSA to conduct NBS and a memorandum of understanding with the Illinois Department of Public Health NBS program to provide follow-up services to parents of newborns with positive SCD or SCT results. SCDAI also partners with the University of Illinois at Chicago sickle cell centers to provide free hemoglobinopathy screenings to more than 500 families, disease self-management training for individuals with SCD, and care coordination training for parents of children with SCD. The organization undertakes philanthropic and charity events, such as bowling and golfing tournaments, to raise awareness and runs an annual toy drive and holiday event to provide gifts to more than 5,000 children living with SCD (SCDAI, n.d.).
Sickle Cell Disease Association of America, Michigan Chapter, Inc.
The Sickle Cell Disease Association of America, Michigan Chapter, Inc. (SCDAAMI) provides education, social work, and care coordination services. The organization works with a psychologist and social worker at the Children’s Hospital to help patients access appropriate services, including career planning, and to navigate relevant Social Security Administration programs. SCDAAMI also has camps for children aimed at fostering independence, and it receives funding from HRSA to run the NBS program in the state. The organization has several support and wellness programs for adolescents living with SCD, including Project Enrich (which provides tutors for students twice per week and offers nutritional education, yoga, and other wellness activities), and the organization also offers homework aid for hospitalized children. SCDAAMI has prepared information to educate legislators. In addition to receiving federal funding for specific programs, SCDAAMI organizes annual fundraising activities, such as walks for SCD (SCDAAMI, n.d.).
Sickle Cell Association of Texas Marc Thomas Foundation
The Sickle Cell Association of Texas Marc Thomas Foundation offers care coordination and case management services, including health
screening, transportation, basic needs assistance, emergency financial assistance, and counseling (Sickle Cell Association of Texas Marc Thomas Foundation, n.d.). The organization also runs a variety of free camps targeted at different age groups, including Camp Next Level, described as a 4-day intense transitional program for 15- to 19-year-olds. The foundation also provides medical case management, screening and education for trait and disease status, and education to professionals (e.g., social workers, clinicians, and teachers) on stigma, prejudice, mental health, and ethics.
Sickle Cell Community Consortium
SCCC is a relatively young organization that originated in the 2014 Patient-Focused Drug Development Initiative from the U.S. Food and Drug Administration (FDA). The consortium was formed to “harness and amplify the power of the patient voice” (SCCC, n.d.). The consortium, in partnership with its sister organization, Sickle Cell Warriors, acts as an organizing entity for SCD CBOs, patient and caregiver advocates, community partners, and medical and research advisers, with the goal of having them work together to identify needs and gaps in the SCD community, strategies to address those needs, and the partners best positioned to implement those strategies (SCCC, n.d.). SCCC’s activities are educational, and its constituents are primarily individuals and CBOs that liaise directly with the SCD population. The consortium’s annual leadership summit convenes patients, caregivers, and CBOs to engage in training opportunities and lectures that are designed to equip and empower them in their advocacy work. The consortium also organizes the annual Sickle Cell Warriors Convention, with input from the patient community, which is designed to educate and empower patients, and also Warrior University, an online repository of educational resources that the SCD population and caregivers curate for the general public. It is unclear from publicly available information how the consortium funds its activities, but its annual meetings are sponsored and supported by industry partners and federal agencies.
Summary
The organizations detailed above have made enormous strides in their states in advancing the policy priorities for the SCD population, and they are making an impact in local SCD communities. Local awareness activities, such as charity walks, runs, and golf outings (especially during September, which is National Sickle Cell Disease Awareness Month, and June, which includes June 19 as World Sickle Cell Day), have still not managed to garner as much national momentum for SCD awareness as has happened for other diseases. This could be attributed to the fact that there is little to no
coordination among national, state, or local organizations. In addition to the state and local SCD agencies listed on the SCDAA and CDC National Resource Directory and in Appendix K, there are many more advocacy groups online, leveraging the power of social media to spread awareness and provide patient support and education to thousands of individuals with SCD and their families.
Individuals with SCD and Their Families Advocating for Themselves
As far as empowerment, first it starts with you.
—Unknown (Open Session Participant)
Self-advocacy is the act of communicating one’s needs within the scope of the issue at hand in order to have them met in a timely and appropriate manner (Ramos Salazar, 2018; Wiltshire et al., 2006). This can be applied in every aspect of life: educational, social, medical, and employment. Successful self-advocacy is based on building effective relationships with the various stakeholders who can influence or meet these needs. In the SCD community, individuals with SCD are often not viewed as “advocates” unless they speak at a conference or participate in a steering committee or professional or governmental working group. However, this belief is misguided; individuals and sometimes their caregivers may be best positioned to represent their own needs and preferences. Self-advocacy is effective because individuals understand their disease, know their body, and can articulate their symptoms, which sometimes may lead to the right diagnosis, pain relief, treatment of the underlying medical condition, and appropriate enabling services to improve QOL (Ramos Salazar, 2018; Wiltshire et al., 2006). For a caregiver’s perspective, see Box 8-1.
Developing self-advocacy skills should begin early in childhood and continue throughout the life course. As discussed in Chapter 2, health literacy limitations, socioeconomic status, race, ethnicity, stigma, and discrimination are all potential impediments to effective self-advocacy for persons living with SCD. These obstacles are further reinforced by the general power imbalance within the health care system, where the power lies with the physician or other health care provider. Even in the realm of “patient-centered care,” where the patient is the key member of the care team, the existing culture means that patients and their families do not have an equal voice in the decision-making process. The medical team is perceived and purported to be in charge, and it ultimately makes the key decisions, thus minimizing the emphasis on patient engagement and shared decision making in care delivery.
Another barrier to self-advocacy may be that at the point of care, in either the emergency department or the hospital, the individual with SCD
may be too incapacitated to be effective. Even when individuals with SCD attempt to effectively self-advocate, they may be disbelieved or referred to as difficult or non-compliant, particularly with respect to pain management. It is not unusual for well-informed and activated individuals to share their individualized pain management plans with providers and, rather than be applauded for being actively engaged and invested in their chronic disease care, be accused of drug-seeking for requesting a specific pain medication, dose, and interval of administration.
The committee was unable to find any studies on self-advocacy in the SCD population. However, the patient and panelists meetings at the committee’s
open sessions underscored the resilience of individuals with SCD, as many of them have been able to leverage their diagnosis to become advocates for themselves and others with the disease. Research from the general patient population shows that patient self-advocacy is a predictor of patient satisfaction and is an essential skill in chronic disease management (Ramos Salazar, 2018; Wiltshire et al., 2006). One study, however, found that the African American women in the study sample were less likely to advocate for themselves than white or Hispanic women by discussing health information that they have obtained with their providers, highlighting an opportunity to equip patients to be better self-advocates (Wiltshire et al., 2006).
Other Organizations Addressing the Needs of the SCD Population
There are myriad other stakeholders that may not be formally recognized as SCD patient advocates but whose functions may confer the same benefits of patient advocacy. For example, health care professional associations may also seek to promote the well-being and interests of the patient. One example of this in SCD is the ASH Sickle Cell Disease Coalition (SCDC)—a disease-focused initiative to address the burden of SCD, both in the United States and globally. ASH established SCDC in 2016 to “help amplify the voice of the SCD stakeholder community, promote awareness, and improve outcomes for individuals with SCD” (ASH, 2017). SCDC is made up of multiple stakeholders in the SCD sphere, including patient advocacy groups. ASH’s activities are multifaceted and include SCD community engagement workshops and focus groups (individuals with SCD in eight cities around the United States) to inform a handbook on the appropriate design and conduct of patient-centered clinical trials (from communications with ASH staff).
Patient advocacy groups that are not specific to SCD but that advocate for individuals with rare and inheritable diseases also contribute to the advocacy efforts for SCD. According to its website, the National Organization for Rare Diseases (NORD) works with its approximately 280 patient member organizations to offer education, advocacy, research, and patient services, with the goal of identifying, treating, and curing rare diseases, including SCD. In addition to advocating for legislation for rare diseases and provider education, NORD offers patient-specific programs, with education for patients and families, and patient services, such as financial assistance for drug access and travel and lodging assistance for clinical trials (NORD, 2020).
The Genetic Alliance is another national organization that supports individuals, families, and communities affected by rare genetic diseases. It advocates for these rare disease populations and connects individuals to advocacy outlets that help make their voices heard. The Genetic Alliance has a research arm that ensures that patient groups and activated communities
are truly leading and driving the research effort. It supports its own bio-bank, institutional review board, patient registry, and engagement platform and provides education and advocacy support for organizations to foster participants becoming research drivers.
CHALLENGES FACED BY SICKLE CELL ADVOCATES AND GROUPS
Individuals and organizations advocating for the population of individuals living with SCD face several obstacles that may limit their effectiveness in accomplishing their goals. The first obstacle, which was alluded to earlier in this chapter, is that many of these organizations operate at the local level and in silos and are thus unable to effect change at the broader level. Currently, none of the SCD CBOs or patient advocacy groups are empowered to influence change for all aspects of the population’s needs, in contrast with groups focused on hemophilia and cystic fibrosis (CF), as discussed later in this chapter. The other barriers pertain to a lack of human and financial resources.
Financial Sustainability
To diversify funding sources for CBOs and SCD advocacy groups, outreach has to be deliberate and focused.
—Derek R. (Open Session Panelist)
The sources of funding for SCD CBOs and patient advocacy groups are few and fail to provide sustainability. These organizations may be funded by federal grants, state entities, the pharmaceutical industry, or charitable events (see Figure 8-3).
Some CBOs and patient advocacy groups receive funding from the federal government in the form of grants for specific projects. In 2017, SCDAA was awarded a $11.6 million, 4-year grant through HRSA (HRSA, 2016); SCDAA also works as the National Coordinating Center to provide technical assistance to 15 CBOs that are sub-awardees to the HRSA grant. The CBOs, including SCFGA, SCDAA–Mobile Chapter in Alabama, Sickle Cell Disease Association of America/Ohio Sickle Cell and Health Association, and the Children’s Sickle Cell Foundation, collaborate with other organizations in their states to conduct NBS follow-up to ensure that individuals diagnosed with SCD are appropriately referred to and are receiving necessary services, such as counseling, education, and other enabling services (SCDAA, n.d.). Grants such as HRSA’s NBS follow-up program are time-bound, so there is no continuity, and funding for the programming
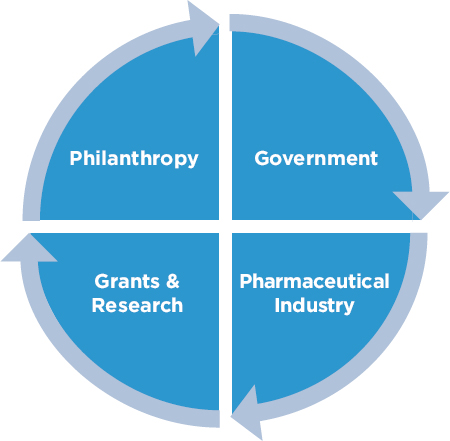
NOTE: Funding from the sources is not proportional.
ends when the grant period does, fostering discontinuity if grants are not renewed. HRSA also funds the five regional collaboratives through the SCDTDRCP. Each collaborative is composed of a range of partners, including CBOs working on the grant goals of improving access to high-quality comprehensive SCD care, provider training, and data collection on SCD quality metrics (PSCRC, 2019).
Collaborative efforts between the two groups are difficult to discern. The role of CBOs within SCDTDRCP varies across the five regional collaboratives. Grant support is usually allocated for specific programs and does not pay for hiring staff or capacity building. The funding available to CBOs through these grants is limited, which promotes competition. The federal grant process also excludes many CBOs because they do not have the appropriate fiduciary infrastructure or staff with the grant writing skills to develop a competitive application in response to a call for proposals.
Some CBOs and patient advocacy groups receive state funding, including SCFGA (Georgia), Piedmont Health Services and Sickle Cell Agency (North Carolina), and SCDAAMI. Most state funds are also for specific programs and do not facilitate capacity building to support the myriad of other services needed by the local SCD population.
The pharmaceutical industry is also a funding source for several SCD CBOs and advocacy groups. Most often, these organizations provide support for specific programs, such as conferences or workshops. For instance,
SCDAAMI lists Sanofi, Genzyme, Emmaus, Pfizer, and other pharmaceutical companies as sponsors on its website (SCDAAMI, n.d.). Certain pharmaceutical companies also have set aside funds that they make available to CBOs through competitive grants. The Access to Excellent Care for Sickle Cell Patients Pilot Program through Global Blood Therapeutics (GBT) is one such example; it provides up to $50,000 during a 12-month period to CBOs and patient advocacy groups serving individuals with SCD and their families with the aim of piloting a variety of models to deliver high-quality health care (GBT, n.d.). Pilots may be focused on expanding CBO capacity by partnering with federally qualified health centers, improving transition from pediatric to adult care, and innovative training programs for clinicians. Novartis also announced the Solutions to Empower Patients (STEP) program in 2018, which provided up to $50,000 to encourage CBOs, patient advocacy groups, and other entities to innovate. The preceding year’s STEP grants were targeted at organizations for metastatic breast cancer (Novartis, 2018), indicating that the funding source is not specific to SCD and likely not a long-term source of funding. Some have highlighted the inherent conflict that CBOs and SCD patient advocacy groups face in relying on pharmaceutical companies because the funds may not support their programmatic needs. Finally, CBOs and patient advocacy organizations may also fundraise through charity events, such as annual galas, sports events, and conferences.
In summary, there are a variety of ways that these CBOs and other nonprofits support their activities. These funding mechanisms are not robust, available funds are limited for a defined range of activities, and they are possibly unable to support much needed organizational development to help CBOs scale their services to reach more individuals. As a result, these funding opportunities may inadvertently lead to mission creep, fragmentation, and inefficiency. It is important that SCD advocacy groups remain mission-focused, but this is a current challenge. Thus, there is a need to diversify funding sources at all levels—federal, state, and private—and to identify dedicated sources of funding that will support sustained programming.
Infrastructure
Most CBOs and patient advocacy groups operate with very few staff and rely on volunteers for their daily operations and activities. The challenge with this model is that programming is contingent on volunteer availability. In 2018 SCFGA reported using 3,990 (750 non-camp) hours of donated time (3–100 hours per volunteer) (SCFGA, 2018). The limited staffing levels also mean that the organization may not have the necessary expertise for its programming, including not having enough adequately
trained staff to provide patient and community education, sufficient CHWs to conduct outreach in the community, the necessary expertise for grant writing and fundraising, or other core capabilities necessary for success. CBOs should have access to technical support that broadens staff skills and services. Programs are needed to support grant writing, budgeting and finances, legal counseling, client engagement, care coordination, and support for research participation.
Individual Challenges
Patient advocates may face a number of challenges as well. Some advocates may be worried that their activities will disrupt their relationship with their health care providers. In a focus group with ovarian cancer patients, for example, those who wanted to self-advocate identified locating relevant health information as one of their major challenges and also expressed hesitation at taking any action that might upset their relationships with their health care providers (Hagan and Medberry, 2016). Yet, data suggest that patient self-advocacy is a predictor of patient satisfaction. A 2018 study of 522 patients found that patients’ education about their disease and their ability to assert their needs positively influenced their satisfaction with their physicians (Ramos Salazar, 2018). This finding has important implications for the SCD population, considering the issues with the patient–provider relationship that were discussed in Chapter 2. Second, advocates often carry out their activities in addition to their current work and life responsibilities. This may lead to their involvement waxing and waning over time, as they may have limited time or energy for advocacy activities at times. Third, advocates living with SCD may find that their health affects their ability to participate in advocacy activities.
MODELS OF PATIENT ADVOCACY FROM OTHER RARE DISEASES
Two diseases referred to throughout this report, hemophilia and CF, offer valuable models for patient advocacy and community engagement for the SCD population. However, the trajectory of these diseases has been different from that of SCD, so these models may not be entirely applicable. Some of what distinguishes these diseases from SCD is the minimal role the pharmaceutical industry has played in SCD, in part because the mainstay drugs for the disease (penicillin and HU) were generic when adopted for SCD. Both hemophilia and CF provide important examples about patient advocacy for rare diseases.
Chelation therapies are the primary agents developed in the past two decades in which the SCD community has interacted directly with
the pharmaceutical industry. It is worth considering how patient advocacy has contributed to the awareness, funding levels for research and patient services, and improvements for individuals living with the conditions and addressing components that could pertain to SCD.
Hemophilia
Hemophilia is an inheritable blood disorder that prevents the blood from clotting, ultimately causing severe bleeding from any minor injury. Because hemophilia has no cure, it requires constant, high-quality care from providers at hemophilia treatment centers (HTCs), which are partially funded by CDC, HRSA, MCHB of HRSA, and other federal agencies. The pharmaceutical industry has partnered with the hemophilia organizations for more than four decades in developing agents to ameliorate hemophilia complications. CDC funding supports programs for research, surveillance, and prevention for bleeding and clotting disorders (NHF, 2020d). HTCs are unique in that they provide comprehensive specialty care for hemophilia and related disorders and also function as an additional resource for a primary care provider (PCP), dentist, or other specialist to ensure best care practices. HTCs provide genetic counseling, medical and psychosocial care, and other services to patients and their families.
The Hemophilia Patient Advocacy Model
The hemophilia patient support landscape is dominated by four well-known organizations: the National Hemophilia Foundation (NHF), the Coalition for Hemophilia B, the Hemophilia Federation of America (HFA), and the World Federation of Hemophilia (WFH) (Azevedo, 2017). As its name suggests, the Coalition for Hemophilia B focuses on treatment and improving the QOL for individuals with hemophilia B. The discussion in this section focuses on the other three organizations whose efforts are targeted at individuals with all forms of hemophilia.
Global efforts
WFH, which leads global advocacy efforts for hemophilia, was established in 1963 to improve care and treatment globally. The founding patient associations for WFH included groups from Argentina, Australia, Belgium, Canada, Denmark, France, Germany, Japan, the Netherlands, Sweden, the United Kingdom, and the United States (WFH, 2020b). WFH established its global presence when it became a member of the World Health Organization in 1969. In 2019 WFH had programs in 22 countries (excluding the United States) in 6 regions of the world, with objectives organized around the six key areas in its comprehensive development model: government support, care delivery, medical expertise and laboratory
diagnosis, treatment products, patient organization, and data collection and outcomes research (WFH, 2020a). WFH’s work in the United States is conducted through WFH USA, its U.S. affiliate. The two entities collaborate on the other WFH programs: humanitarian aid, research and data collection, and training and education. As part of the humanitarian aid program, WFH distributes donated pharmaceutical products to individuals with hemophilia in developing nations. The World Bleeding Disorders Registry (WBDR), a longitudinal, prospective patient registry that provides patient-level clinical and outcome data, was established in 2018 as part of WFH’s research and data collection efforts. WBDR issued its first report in May 2019 (WFH, 2020c). WFH uses WBDR data collected to strengthen its efforts to educate key stakeholders and generate awareness about the needs of the hemophilia population (WFH USA, 2020). Finally, WFH training and education efforts focus on training health care professionals and community leaders through workshops delivered primarily through its eLearning platform.
WFH and WFH USA’s work is bolstered by in-kind medication and financial donations by partners such as Sanofi Genzyme, Sobi, CSL Behring, GC Pharma, and Grifols (WFH USA, 2018). Products donated to WFH and WFH USA in 2018 totaled approximately $378 million. Financial donations from corporate and community partners in 2018 totaled approximately $1.57 million (WFH USA, 2018). WFH USA partners with members of NHF through the NHF Chapter Challenge, which asks NHF chapters to provide support for the WFH humanitarian aid program. Since its launch in 2016, the NHF Chapter Challenge has raised $482,462 (WFH USA, 2018).
Efforts in the United States
The other two main organizations working to support individuals with hemophilia in the United States are NHF and HFA. Established in 1948, NHF is the oldest organization advancing awareness and promoting better treatment and cures. It is believed to have made substantial contributions to improving awareness for hemophilia, including advocating for more resources for research, encouraging access to high-quality care, and providing patient and family support.
When the organization was established, the life expectancy for hemophilia was approximately 30 years; with access to appropriate therapy, life expectancy is now normal. NHF has a national, state, and local presence through its 51 nationwide chapter affiliates, 7 of which are owned by the foundation (NHF, 2017).
At a broader level, NHF and chapter organizations’ activities focus on ensuring better treatments and a cure for inheritable bleeding disorders through education, research, and advocacy. NHF has initiatives in state and federal legislation on access to health care, payer education, educating workers and the public, and other advocacy issues. The foundation also promotes shared decision making between physicians and patients, family
support networks that pair patients with mentors for peer support, community groups that provide support and education, and self-infusion. At the state level, NHF monitors issues of priority to the hemophilia population, such as Medicaid-managed care to ensure that costs remain affordable (NHF, 2020a). It also provides training and strategic planning courses to state hemophilia chapters and coalitions.
NHF has been instrumental in advancing the organization and delivery of high-quality care nationwide. In 1973 NHF spearheaded a 2-year campaign that led to creating the network of comprehensive HTCs (NHF, 2020b). Currently, there are 141 HTCs that are part of the U.S. Hemophilia Treatment Center Network providing comprehensive care to individuals with hemophilia throughout the United States and its territories (CDC, 2018a) (see Chapter 5 for the hemophilia care model). Since 1974, Congress has supported the HTCs through HRSA to provide “comprehensive multidisciplinary services not typically covered by insurance, such as physical therapy assessments, social work, and case management services,” and through CDC to “support research, surveillance, and prevention for bleeding and clotting disorders, including hemophilia” (NHF, 2020d). The NHF Medical and Scientific Advisory Council (MASAC), a group of expert scientists, physicians, allied health professionals, patients, and government liaisons from the relevant federal agencies within the U.S. Department of Health and Human Services, advances the standard of clinical care and issues treatment recommendations for all bleeding disorders (NHF, 2020c). “MASAC guidelines [issued as recommendations] set the standard of care and are frequently referred to by an international array of physicians, medical schools, pharmacists, emergency room personnel, insurance companies, patients, and others” (Skinner et al., 2014, p. e545).
NHF also promotes the interests of individuals with hemophilia and their families by partnering with affiliated chapters to develop policy agendas at the federal and state levels on issues pertaining to “improved access to high-quality medical care, a safe blood supply, access to the full range of safe and effective treatments, adequate reimbursement at the public and private levels, and expanded federal funding for hemophilia treatment centers” (NHF, 2020c). These agendas are used to guide the organization’s educational, policy making, and public awareness campaigns and other activities. NHF supports chapters in serving their local communities, including liaising to build relationships between chapters and HTCs, providing grants for educational programs and staffing, and assisting with grant writing. NHF also offers national, regional, and local training to chapters (NHF, 2020c).
According to its 2017 financial statements, NHF’s activities are funded primarily by pharmaceutical companies (82 percent of revenues) (NHF, 2018), and the organization has reported net assets of $23,210,450.
HFA was established in 1994 to “address the evolving needs of the bleeding disorders community” (HFA, n.d.), triggered by the contamination of blood products in the late 1970s through mid-1980s with HIV and the hepatitis C virus (HCV), which posed a particular burden for individuals with bleeding disorders. In the 1980s approximately 90 percent of people with severe hemophilia were infected with HIV, and almost all people living with hemophilia who used factor products before 1988 were infected with HCV, complicating their care (HFA, n.d.). HFA’s goal was to create a voice for the patient in light of this devastation to the hemophilia population. Many of HFA’s programming and educational activities mirror those undertaken by NHF. In fact, the majority, if not all, of the 40 state and local CBOs that are HFA members are also part of NHF. NHF and HFA release joint statements on key policy issues pertaining to the hemophilia population and in accordance with their missions. The reported net assets for HFA in 2017 were $5,422,183 (HFA, 2017). In 2010 the HFA board of directors reversed the association’s stance of refusing funding from pharmaceutical companies producing therapeutic products for hemophilia; it currently lists Takeda, Genentech, Bayer Healthcare, CSL Behring, Novo Nordisk, Sanofi Genzyme, HEMA Biologics, Kedrion Biopharma, and Pfizer Rare Disease among its top supporters.
Key Takeaways from Hemophilia Patient Organizations for SCD
There are factors that have contributed to the effectiveness of CBOs and national organizations serving the hemophilia population. Some of these may not immediately be applicable to SCD organizations, but hemophilia organizations had to overcome challenges with public awareness, patient and provider education, lack of funding, and accessing high-quality, comprehensive care similar to those that now confront the SCD population, so there are some worthy takeaways that could inform the patient advocacy landscape for SCD.
Defined leadership and concerted efforts
There are several organizations working independently to promote research, education, and care and to meet the overall needs of individuals with hemophilia, but the three organizations discussed in this section emerge as leading these efforts in the United States and globally. CBOs that support the needs of children and adults with hemophilia and their families at the state and local levels also work closely with these organizations to ensure a unified voice in messaging and education to policy makers, providers, and other relevant stakeholders. NHF is also influential in informing high-quality care through MASAC, which sets clinical guidelines. The coordinated efforts of hemophilia organizations are evident even at the state level, as demonstrated by the Hemophilia Council
of California (Hemophilia Council of California, n.d.). SCD CBOs and their patient advocacy efforts are currently siloed, with no organizational model of how the national, state, local, and virtual organizations are working together to address the shared goal of advancing important issues. The result is duplicated efforts, diversification of the limited resources that exist, and a lack of a unified voice and message in support of the SCD population.
Funding
In 2018 there were an estimated 28 different hemophilia drugs available in the United States, with another 21 in development (Terry, 2018). The number of pharmaceutical companies engaged in therapeutic development for hemophilia is a source of support for the relevant CBOs and patient advocacy groups. The public awareness that hemophilia has gained over the decades has also translated into additional financial support for research and other activities.
In contrast, most funding for SCD patient advocacy is from federal sources in the form of grants for specific projects rather than organizational development, capacity building, and programming. Some pharmaceutical companies, such as GBT and Novartis, are funding SCD CBOs’ work, but these funds are still limited, competitive, and available to only a few organizations. There is the potential for diversified sources of financial support—both private and federal—for SCD patient organizations. Public awareness, education, and understanding of SCD and the burden on the community could generate more private-sector support for SCD organizations. As mentioned, the lack of a defined model of organization and centralized leadership for SCD CBO efforts is a potential impediment.
Role within the care delivery system for hemophilia
Creating HTCs and the definition of standards of care delivered by HTCs established hemophilia CBOs as part of the hemophilia ecosystem. Standards and Criteria for the Care of Persons with Congenital Bleeding Disorders, published by NHF’s MASAC, identifies opportunities to engage CBOs in health care (NHF, 2002). For example, the standards call for enhanced communication among the health care team and patients, consultants, PCPs, and other community-based health care workers to support the patient’s needs; for the establishment of a community network to link CBOs with HTCs to maximize resources and minimize duplication of services; and for referrals from HTCs, with the consent of the patient, to social services and CBOs that are positioned to address basic human needs, such as food, clothing, and transportation (NHF, 2002). Currently, SCD CBOs operate in parallel with the health care system. Health system–based social workers and CHWs provide supportive functions to individuals living with SCD, but most are also mired in administrative activities, care for a full panel of patients, and are unable to dedicate sufficient attention to SCD individuals’ needs. CBOs
and their staff are best positioned to support their patients as they transition out of the health care system into the community. However, there is a void between the health system and the community-based resources that partially results from the lack of a unified effort among organizations serving the SCD population, thereby making it difficult to identify the appropriate CBOs for handoff. A well-defined model of organization for CBOs and other organizations will streamline efforts and offer guidance for how to leverage their capabilities in the comprehensive care model proposed by the committee in this report.
Policy and historical impetus for action
Finally, it is worth noting that several policy and historical events have contributed to the effectiveness of hemophilia patient advocacy and community groups. Congress authorized funding in 1975 to establish comprehensive hemophilia clinics, which was later expanded; that was influenced by—but also spurred on—the efforts to improve care and outcomes. The AIDS and hepatitis C crises in the later 1970s and the 1980s also galvanized efforts by creating urgency for improved testing for clotting agents and empowering individuals living with hemophilia and communities to advocate for themselves (Baker et al., 2005). These events cannot be replicated for SCD, but SCD may be at a tipping point. CBOs and patient groups are best positioned to engage with the efforts related to several therapeutic products in the pipeline, the move for universal curative therapies (which will necessitate patient and provider education about scientific developments to inform treatment decision making), and the need to ensure access to beneficial therapeutic products that will soon arrive on the market.
Cystic Fibrosis
The CF community is small but highly active, thanks in part to the national patient advocacy group. The Cystic Fibrosis Foundation (CFF) was established in 1955, when affected individuals were not expected to survive childhood. As of 2012, life expectancy was approximately 41 years because of CFF’s activities to find a cure and prolong healthy lives (CFF, n.d.f; Mogayzel et al., 2014). CFF leads efforts to improve care, to increase access to beneficial therapies, to increase public education and awareness, and to improve the delivery of support services. CFF differs from other patient advocacy groups in that it directly oversees aspects of the care organization and of the delivery, data collection, therapeutic product development, and services for health-related social needs.
The CF Care Center Network was established in 1961 when CFF accredited two CF centers based on criteria established by its center committee, which developed the standards for care, research, and teaching
that each center must implement and sustain for accreditation. These requirements included convening a team of experts to treat inpatient and outpatient clinical needs, implementing care guidelines developed by CF clinical experts, and treating people with CF to improve the knowledge of the center’s medical team (Mogayzel et al., 2014). In 2019 there were more than 130 care centers (CFF, n.d.b), which are reviewed each year and undergo periodic visits from the center committee to maintain accreditation. CFF also funds care centers to enable them to participate in clinical research and in training multidisciplinary care teams about clinical best practices.
In 1966 CFF created a patient registry to collect data with which to track the impact of the CF care standards on individuals’ health. Providers at the care centers enter health data on consenting patients. Today the patient registry provides key information to the care centers and the CF community about the natural history of the disease, its complications, the impact of care delivery, and important clinical outcomes. This information feeds into the creation of a learning health system, where real-time data are used to refine and improve clinical care. Factors identified as important for survival, such as CF-related diabetes, nutrition, and lung function, then inform the quality improvement efforts at the care centers (Mogayzel et al., 2014).
CFF launched into drug development in 2000 when it provided investments to the first pharmaceutical manufacturer to conduct research to identify compounds that might alter genetic errors in people with CF (CFF, n.d.c). This investment began CFF’s venture philanthropy model for drug development. The impetus for this model was the lack of progress made by the late 1990s in developing therapeutic products that addressed the underlying cause of the disease (CFF, n.d.c). As is the case with most rare diseases, most pharmaceutical companies were reluctant to invest time and resources into clinical research to identify therapies that would benefit only a small population. The venture philanthropy model was CFF’s response to that obstacle: funding drug development with for-profit companies. Since the initial investment, CFF has funded several biopharmaceutical companies, including Pfizer, Genzyme, Editas, and Corbus, and invested $425 million to accelerate drug development for CF (CFF, n.d.c). CFF’s investment has led to the approval of several drugs, with many more in the pipeline (CFF, n.d.e). The venture philanthropy model has also funded CFF for further research, the care centers, and services to the CF population. CFF enters into agreements with drug companies in which it invests to receive royalties related to drugs developed as a result of its funding (CFF, n.d.e). This model, with CFF taking the lead in funding drug development and using the payoff from its investments to underwrite its activities, is unique because the drug development function has traditionally been kept
separate from other functions in health care in order to protect the patient’s interests.
The drug development process is the main source of funding for CFF. In 2014 CFF “sold royalty rights for CF treatments developed by Vertex for $3.3 billion” (CFF, n.d.c), making it the nation’s largest disease-focused charity by net assets (Tozzi, 2015). In 2018 CFF also raised more than $80 million from the CF community in the form of charity events, such as walks and golf outings (Tozzi, 2015).
CFF is actively involved in funding health-related services for individuals with CF and their families through its Compass program, which helps individuals with CF navigate insurance requirements; identify financial resources to defray copays, deductibles, and other financial obstacles to accessing care; apply for benefits, including Social Security and disability; acquire legal information for employment, education, and other government benefits; and identify resources to address a variety of social determinants of health, including transportation to and from care, and housing, living, and food expenses (CFF, n.d.d).
CFF works with its 70 chapters and branch offices across the country to raise funds and support the CF community. However, it is unclear from the publicly available information how the chapters are organized and operate in conjunction with CFF.
CFF, care centers, and chapters are actively involved in generating awareness and working at all levels of government to shape public policy and increase awareness resources. At the federal level CFF has pushed for expanded funding for NIH and FDA to support basic and translational research and requested greater resources for the drug approval process, which increases the chances of finding a cure. At the state level, CFF joined forces with CF care centers and patient advocates around the United States to rally for programs like Medicaid to express the need for constructive insurance coverage policies for care and therapies. The organization spoke to lawmakers about the complications of CF and the need for access to the appropriate treatments. In addition, it also turned its focus to legislation that influenced health programs essential to high-quality CF care (CFF, n.d.a).
Public awareness of CF has been bolstered by the influence of high-profile personalities. Canadian singer Celine Dion has been an advocate, dedicating her time and money to the CF community in Canada for more than 30 years (Global Genes, 2015). The tragic loss of her niece at the age of 16 to CF sparked her to become an advocate for the CF community. She has appeared in multiple CF campaigns and is a known advocate for CF NBS. Dion has pressed lawmakers to support efforts for NBS through service announcements and public appearances, hosted benefit concerts and galas, and donated much of her personal funds toward research and awareness (Global Genes, 2015). During his 2015 State of the Union address,
President Obama “cited the story of CF as an example of how nonprofits, the pharmaceutical industry, researchers, patients, and their families can work together to produce more targeted and effective treatments for diseases” (CFF, n.d.c).
Key Takeaways from Cystic Fibrosis Patient Organizations for SCD
The CFF model of patient advocacy is unique in its scope of activities and also reflects a model for how patient advocacy groups can drive efforts in response to the perceived needs, as opposed to change being driven by external factors. This model is not entirely replicable because of the level of risk that the organization assumes. The CFF venture philanthropy model is now emulated by organizations for other rare diseases, and NIH has adopted CFF’s strategies to advance drug development for rare diseases.
The influx of pharmaceutical companies into therapeutic development for CF means that this approach is probably not warranted for SCD. However, there is an opportunity for CBOs and other organizations working to create awareness for and address the needs of the SCD population to actively define and shape the provision of high-quality care for the SCD population. Some organizations, such as ASH, have taken steps by developing clinical practice guidelines for SCD care, but there is currently no mechanism to translate these guidelines into practice (see Chapter 6). The disparate efforts under way with multiple organizations are also a potential barrier to meaningfully influencing care, outcomes, and change for the SCD population.
OPPORTUNITIES TO MOVE FROM LOCAL TO SYSTEM-LEVEL CHANGE
If you’re going to advocate for something, I would advocate for more than minimal.
—Amy S. (Open Session Panelist)
Patient advocacy groups and CBOs clearly play an integral role in SCD, providing the necessary health-related services; educating individuals and their families, providers, legislators, and other key stakeholders; and helping to generate awareness in the process. There is an opportunity to leverage these organizations as key stakeholders in any action to improve care and outcomes, especially in delivering the comprehensive, person-centric care that the committee recommends. There are four opportunities to establish CBOs and patient advocacy groups as key stakeholders in SCD action.
Integrate Community-Based Organizations and Advocacy Groups as an Integral Part of the Care Delivery Process
You have to have support; even if you don’t have family that understands, having a community of support is integral.
—Tosin O. (Open Session Panelist)
CBOs and patient advocacy groups are already actively contributing to the care delivery process, from the initial stages (identifying individuals who screened positive for SCD or SCT for clinical follow-up), to CHWs entering the community to assist individuals who are unable to reach care, to providing education to help individuals manage their care. This role can be strengthened through formalized handoffs from the health care system to the community and vice versa. Health system–based CHWs and social workers primarily assist individuals with navigating insurance and scheduling appointments. However, their role does not extend into the community because they cannot follow individuals after they leave the health care system. CBOs could take over once a person is back in the community. Formal handoffs will ensure that no one is lost after departing the health care system. By having a community partner assist, individuals with SCD may also be able to effectively manage their care and minimize disease complications.
Leverage Community-Based Organizations and Advocacy Groups to Address the Social Needs of Individuals Living with SCD
There is also an opportunity to leverage the strength of CBOs and advocacy groups in addressing the social and health-related needs of individuals with SCD and their families. Most CBOs are already addressing these needs but are limited in their ability to do so due to the aforementioned challenges.
Integrate Community-Based Organizations and Advocacy Groups into Clinical Trials and Research Processes
It is necessary to create opportunities for advocacy groups to be an important part of the care delivery and research process—from helping to inform clinical trial design and recruitment to facilitating patient access to health care services.
| Advocacy and Awareness | Genetic Counseling and Screening Education | Direct Enabling Services | |
|---|---|---|---|
| Tier A | Engage a professional in lobbying efforts as a consultant or staff | Health professional for oversight of certified genetic counselors’ onsite screening; organized education and oversight for genetic counseling | Care coordination, referral to medical home, transportation, and other resources |
| Tier B | Organize state-level advocacy efforts | Trait testing on site, state newborn screening follow-up, and certified genetic counselors | Transportation services, case finding, and referral to medical home |
| Tier C | Hold periodic local awareness events | Referral to state department for testing and education about sickle cell disease/sickle cell trait | Referrals to community resources |
Standardize Structure for SCD Community-Based Organizations and Patient Organizations
There is a need for a system that classifies SCD CBOs according to the type and breadth of services provided. Table 8-2 categorizes the range of services that CBOs may provide, including advocacy and awareness (e.g., health fairs, SCD/SCT awareness events, national lobbying), education and counseling (e.g., trait testing on site, NBS tracking and follow-up referrals, health professional on site to provide complex genetic counseling), direct enabling (e.g., direct care coordination, transportation, funeral support, utilities), and a combination of any of the above. These services are arranged in tiers, with Tier A representing the highest level and breadth of service delivery. (A CBO in Tier A could also incorporate components from Tiers B and C.)
Classifying CBOs by their capabilities and activities also streamlines outreach by patients, funders, and health care systems, which are able to identify the patient organizations best positioned for different functions. Finally, a classification system could eliminate the siloing of CBOs and SCD patient organizations by helping those performing different functions to learn from each other and share best practices. The absence of a unified voice is one reason for a lack of meaningful impact at a broader level for SCD advocacy groups.
SUMMARY
This chapter summarizes the historical context surrounding the establishment of the SCD CBO and patient advocacy groups for SCD and describes the evolving landscape of SCD CBOs, with a combination of the
traditional CBO model, hybrid models that include individual advocates and support groups, and a primarily virtual model. The chapter also details the various services and initiatives currently in the scope of work of SCD CBOs and patient groups, underlining the fact that there is currently no formal classification system or standardization process of protocols that is universally used among these organizations. Because SCD is by its nature influenced by stigma, racism, and discrimination, this report is not complete without a uniquely defined role for the cultural brokers within the SCD community, the CBOs, or patient advocates.
The committee acknowledges that SCD CBOs provide enabling services that support the physical, mental, and social health of individuals affected by SCD; however, despite their critical importance in the cultural brokerage ecosystem, SCD CBOs are primarily under-resourced in the African American community, underfunded, and dependent on fundraising for their existence, as the business model is focused more on finding funds than on planning activities and then seeking funding sources consistent with those activities. There is a need to identify a sustainable funding mechanism to support the continued existence of SCD CBOs in order to reverse the current fragmentation resulting from a lack of sustainable funding and a standard classification system. CBOs will need a concerted initiative to build consistent and measurable infrastructure, to develop a clear definition of their scope of services based on infrastructure capacity, and build the necessary skills to foster the sustainability of the newly acquired infrastructure.
Finally, an SCD CBO will best thrive in an environment of trust, respect, and equal partnership with other stakeholders in the SCD community. Currently, SCD CBOs struggle to gain recognition from health care systems, state health departments, and local hospitals, largely due to variations in services, an under-resourced infrastructure, and a lack of transparency regarding governance, mission, and fiduciary responsibility. This creates challenges for partnerships at every level, leading to a vicious cycle of continued lack of funding and resources. There is criticism over what SCD CBOs do not provide for their communities when very few have access to the skills and resources needed to brand their organizations, publicize their work, and publish data on their programs. When hospitals do not trust CBOs to provide enabling services and social support, the hospitals work to create them internally. This further stresses the partnerships between stakeholders and CBOs because hospital-based entities are competing for funding through grants and philanthropy.
These challenges are not unique to the SCD community. Therefore, solutions from other chronic diseases should be considered when trying to plan future efforts. One of the initial steps to improving the ability of SCD CBOs to develop long-lasting, proactive partnerships will be to rely on a national organization that can validate their capabilities and services. This
organization could be similar to NHF in structure, provide funding and technical assistance to local member CBOs according to a classification system, and meet certain criteria, including those based on the skill sets of CBO staff. The certification of genetic counselors and CHWs, already existing for SCD, could be expanded and incorporated into criteria for accreditation, with the appropriate required recertification to remain up to date in the knowledge base and the appropriate oversight to ensure counseling competency.
Ideally, this national organization would work to build relationships with other community members, such as health care systems, thereby facilitating partnerships at the local level that would be strategically positioned in communities that contain large numbers of individuals living with SCD. If an organization develops infrastructure, outlines mission-driven programs and services with transparent measurable objectives, trains and certifies staff, and receives accreditation from the national organization, that will bolster the foundation for building a healthy respectful partnership. Maintaining certification and accreditation will require a bidirectional flow of funds between the local and the national organizations. However, federal, private industry, third-party payers, and health system funding, primarily driven from the national level down, will alleviate some of the burden for fundraising at the local level. Quality metrics developed for accreditation will encourage SCD CBOs to collect and store programmatic and service data for reporting. This will help in making CBO-specific data public so that individuals living with SCD can identify the CBOs that provide the services they need. This information will be useful for not only consumer use but also organizational strategic planning, policy development, branding, and marketing. This would further “legitimize” the SCD CBOs among SCD stakeholders broadly and help establish CBO participation in SCD learning networks as valid team members in service provision, patient engagement, and information dissemination.
Community expectations for SCD CBOs are daunting (see this chapter’s introduction). Developing the capacity of the national organization for technical assistance in all areas will require tremendous commitment, dedication, resources, and funding. In the past, funding at the national and local levels for SCD programming and initiatives has come through grants and direct gifts, which are difficult to sustain due to competition. The SCD community will realize that collaboration and partnership must culminate in supporting one or two national or “umbrella” CBOs. The CF and hemophilia communities have handled this well, and available funding is robust. However, in the SCD community funding is sparse, largely due to the minimal development of drugs and technologies. When adopted for use in SCD, penicillin and HU were generic, and procedures (e.g., apheresis) and laboratory tests (e.g., high-performance liquid chromatography) were
fully developed. Recently, SCD drug development has soared. This provides an opportunity for new resources and funding mechanisms for CBOs. All stakeholders might benefit if a well-positioned national organization were to establish a transparent mechanism to fund virtual and local CBOs and measure, monitor, and track how they help children and adults with SCD.
Role of the SCD Community-Based Organization in a National Awareness Campaign
Education and awareness gaps remain in the SCD community, and there is a dire need for robust educational campaigns to address this limited understanding about the origins, impact, and consequences of SCD and the difference between SCD and SCT to avoid a recurrence of the damage done in the 1970s by the poor planning and execution of the SC clinics. An awareness campaign is clearly necessary, in part to dispel the myth in the African American community and beyond that SCD has “gone away” because they do not hear about it anymore. CBOs could play a key role, particularly if a unified message adopted by all stakeholders could be used as the primary campaign message.
The attention that new drugs and curative therapies will bring could be harnessed into messaging, thus procuring funding and resources from private industry. A well-designed campaign would be broad, dispel myths and stigma, attract positive attention, and work to unite the community. Recent media attention has not resulted in positive feedback from adults with SCD and caregivers of children. Awareness “messaging” will require full participation from those affected by SCD, those working toward improving their QOL, and media and news production professionals who understand the African American and Latinx American communities to determine how messaging may be best received by the public. In the interim, targeting inclusion in other public awareness campaigns will improve exposure. For example, CDC sponsors a campaign, Self-Management Education: Learn More, Feel Better, to increase public awareness of disease self-management education that could easily incorporate SCD (CDC, 2018b).
Targeting dissemination in the SCD community would increase awareness of self-management education in the community and also the visibility of SCD in the broader CDC and U.S. chronic illness community. Another example is the #MAKEITVISIBLE movement of the U.S. Pain Society (U.S. Pain Foundation, 2017). Improving the ability to partner with others in chronic illness awareness may benefit the SCD community and foster partnerships at the national and local levels.
National and local projects to raise awareness should identify and address barriers at each level: individuals with SCD and their families, systems of care, and urban and rural communities. Literacy skills and unequal
access to resources must be considered. Campaigns should be within the framework of health promotion but tempered with compassion when discussing prevention, so as not to further stigmatize those living with SCD. National mass media campaigns should be synergistic and consistent with longer-term local CBO action and patient engagement initiatives.
Finally, it is important to recognize the role of the virtual SCD CBO and advocacy groups in supporting awareness, advocacy, and education to help eliminate the isolation that individuals with SCD experience around not just their disease but being involved with and invited to participate in interventions to improve and support SCD. The mantra “Nothing for us without us” should be taken literally when addressing a strategic plan and action blueprint for SCD. There are a vast number of “invisible warriors,” individuals living with SCD and SCT who are not in formal advocacy or community groups but find their sense of community via Facebook, Instagram, Snapchat, and other virtual platforms. They are the informal grassroots network of SCD advocates who should intentionally be sought out, albeit via nontraditional means, and their voice should be included in defining the way forward.
CONCLUSIONS AND RECOMMENDATIONS
Conclusion 8-1: SCD CBOs provide enabling services that support the physical, mental, and social health of individuals affected by SCD; however, despite their critical importance in the cultural brokerage ecosystem, SCD CBOs are primarily under-resourced in the African American community, under-funded, and dependent on fundraising for their existence, as the business model is focused more on finding funds than planning activities and finding funding sources consistent with those activities.
Conclusion 8-2: Funding mechanisms for SCD CBOs and patient organizations are not sustainable and competitive.
Conclusion 8-3: The current organization and structure of SCD CBOs is fractured and fragmented, thereby resulting in inefficiencies and duplication of activities. There is a need for a clear definition of scope of services based on infrastructure capacity and skill building to foster the sustainability of the newly acquired infrastructure.
Conclusion 8-4: Despite the role they play in serving as a liaison between the health system and community resources for individuals with SCD, currently SCD CBOs struggle to gain recognition from health care systems, state health departments, and local hospitals, largely due to variation in services, under-resourced infrastructure,
and transparency regarding governance, mission, and fiduciary responsibility.
REFERENCES
ASH (American Society of Hematology). 2017. About the sickle cell disease coalition. http://www.scdcoalition.org/about.html (accessed July 20, 2020).
Azevedo, M. 2017. 4 hemophilia support organizations you should know about. Hemophilia News Today, August 3. https://hemophilianewstoday.com/2017/08/03/8566 (accessed April 20, 2020).
Baker, J. R., S. O. Crudder, B. Riske, V. Bias, and A. Forsberg. 2005. A model for a regional system of care to promote the health and well-being of people with rare chronic genetic disorders. American Journal of Public Health 95(11):1910–1916.
Bakker, A., P. G. Van der Heijden, M. J. Van Son, R. Van de Schoot, and N. E. Van Loey. 2011. Impact of pediatric burn camps on participants’ self esteem and body image: An empirical study. Burns 37(8):1317–1325.
Bultas, M. W., A. D. Schmuke, V. Moran, and J. Taylor. 2016. Psychosocial outcomes of participating in pediatric diabetes camp. Public Health Nursing 33(4):295–302.
CDC (Centers for Disease Control and Prevention). 2018a. HTC population profile. Atlanta, GA: Centers for Disease Control and Prevention.
CDC. 2018b. Self-management education (SME) programs for chronic health conditions. https://www.cdc.gov/learnmorefeelbetter/programs/index.htm (accessed May 16, 2019).
CDC. 2019a. California SCDC program data. https://www.cdc.gov/ncbddd/hemoglobinopathies/scdc-state-data/california.html (accessed May 16, 2019).
CDC. 2019b. Sickle cell disease national resource directory. https://www.cdc.gov/ncbddd/sicklecell/map/map-nationalresourcedirectory.html (accessed May 16, 2019).
CFF (Cystic Fibrosis Foundation). n.d.a. Advocacy achievements. https://www.cff.org/About-Us/Our-Approach-to-Federal-State-and-Local-Policy/Our-Advocacy-Work/Advocacy-Achievements (accessed January 13, 2020).
CFF. n.d.b. Care centers. https://www.cff.org/Care/Care-Centers (accessed January 13, 2020).
CFF. n.d.c. CF foundation venture philanthropy model. https://www.cff.org/About-Us/About-the-Cystic-Fibrosis-Foundation/CF-Foundation-Venture-Philanthropy-Model (accessed January 13, 2020).
CFF. n.d.d. What is compass? https://www.cff.org/Assistance-Services/About-Compass/What-Is-Compass (accessed July 20, 2020).
CFF. n.d.e. Drug development pipeline. https://www.cff.org/Trials/pipeline (accessed January 13, 2020).
CFF. n.d.f. Our history. https://www.cff.org/About-Us/About-the-Cystic-Fibrosis-Foundation/Our-History (accessed January 13, 2020).
DiDomizio, P. G., and A. Gillard. 2018. Perceptions of health care professionals on the effects of residential summer camp in their patients. Journal of Pediatric Nursing 40:37–46.
GBT (Global Blood Therapeutics). n.d. Access to Excellent Care for Sickle Cell Patients pilot program (ACCEL). https://www.gbt.com/patients/funding-and-support (accessed April 20, 2020).
Global Genes. 2015. RARE on the red carpet: Celine Dion pitches in for cystic fibrosis. RARE Daily, January 25. https://globalgenes.org/2015/01/25/rare-red-carpet-celine-dion-pitches-cystic-fibrosis (accessed April 20, 2020).
Gold, J. 2017. Sickle cell patients suffer discrimination, poor care—and shorter lives. https://mlk50.com/sickle-cell-patients-suffer-discrimination-poor-care-and-shorter-lives-f85abe11bb67 (accessed January 13, 2020).
Hagan, T. L., and E. Medberry. 2016. Patient education vs. patient experiences of self-advocacy: Changing the discourse to support cancer survivors. Journal of Cancer Education 31(2):375–381.
Hemophilia Foundation of California. n.d. About. https://www.hemophiliaca.org/about (accessed January 13, 2020).
HFA (Hemophilia Foundation of America). 2017. 2017 annual report. Washington, DC: Hemophilia Federation of America.
HFA. n.d. What is HFA? https://www.hemophiliafed.org/our-role-and-programs/what-is-hfa (accessed January 15, 2020).
HRSA (Health Resources and Services Administration) Maternal and Child Health Bureau. 2016. Sickle cell disease newborn screening follow-up program. https://www.hrsa.gov/library/sickle-cell-disease-newborn-screening-follow-program (accessed April 20, 2020).
Hsu, L. L., N. S. Green, E. Donnell Ivy, C. E. Neunert, A. Smaldone, S. Johnson, S. Castillo, A. Castillo, T. Thompson, K. Hampton, J. J. Strouse, R. Stewart, T. Hughes, S. Banks, K. Smith-Whitley, A. King, M. Brown, K. Ohene-Frempong, W. R. Smith, and M. Martin. 2016. Community health workers as support for sickle cell care. American Journal of Preventive Medicine 51(1 Suppl 1):S87–S98.
Manley, A. F. 1984. Legislation and funding for sickle cell services, 1972–1982. American Journal of Pediatric Hematology/Oncology 6(1):67–71.
Markel, H. 1992. The stigma of disease: Implications of genetic screening. American Journal of Medicine 93(2):209–215.
Mogayzel, P. J., J. Dunitz, L. C. Marrow, and L. A. Hazle. 2014. Improving chronic care delivery and outcomes: The impact of the cystic fibrosis care center network. BMJ Quality & Safety 23(Suppl 1):i3.
Narcisse, L., E. A. Walton, and L. L. Hsu. 2018. Summer camps for children with sickle cell disease. Ochsner Journal 18(4):358–363.
NHF (National Hemophilia Foundation). 2002. Standards and criteria for the care of persons with congenital bleeding disorders. https://www.hemophilia.org/Researchers-Healthcare-Providers/Medical-and-Scientific-Advisory-Council-MASAC/MASAC-Recommendations/Standards-and-Criteria-for-the-Care-of-Persons-with-Congenital-Bleeding-Disorders (accessed January 15, 2020).
NHF. 2017. 2017 annual report. New York: National Hemophilia Foundation.
NHF. 2018. 2017 annual report. https://www.hemophilia.org/sites/default/files/document/files/Accomplishments_2017.pdf (accessed July 20, 2020).
NHF. 2020a. Advocacy & healthcare coverage. https://www.hemophilia.org/Advocacy-Healthcare-Coverage/Advocacy-Priorities (accessed January 15, 2020).
NHF. 2020b. Comprehensive medical care: Htcs. https://www.hemophilia.org/Researchers-Healthcare-Providers/Comprehensive-Medical-Care-Hemophilia-Treatment-Centers (accessed January 15, 2020).
NHF. 2020c. Fast facts. https://www.hemophilia.org/About-Us/Fast-Facts (accessed January 15, 2020).
NHF. 2020d. Federal hemophilia programs. https://www.hemophilia.org/Advocacy-Healthcare-Coverage/Advocacy-Priorities/Federal-Priorities/Federal-Hemophilia-Programs (accessed January 15, 2020).
NORD (National Organization for Rare Diseases). 2020. Programs and services. https://rarediseases.org/about/what-we-do/programs-services (accessed January 15, 2020).
Novartis. 2018. Novartis to fund five innovative ideas to support patients and the sickle cell community. https://www.pharma.us.novartis.com/news/media-releases/novartis-fund-five-innovative-ideas-support-patients-and-sickle-cell-community (accessed January 15, 2020).
Otero-Sabogal, R., D. Arretz, S. Siebold, E. Hallen, R. Lee, A. Ketchel, J. Li, and J. Newman. 2010. Physician–community health worker partnering to support diabetes self-management in primary care. Quality in Primary Care 18(6):363–372.
PHCPI (Primary Health Care Performance Initiative). 2018. Community engagement. https://improvingphc.org/community-engagement (accessed March 11, 2020).
PSCRC (Pacific Sickle Cell Regional Collaborative). 2019. About. https://pacificscd.org/about (accessed January 15, 2020).
Ramos Salazar, L. 2018. The effect of patient self-advocacy on patient satisfaction: Exploring self-compassion as a mediator. Communication Studies 69(5):567–582.
Rhodes, S. D., K. L. Foley, C. S. Zometa, and F. R. Bloom. 2007. Lay health advisor interventions among Hispanics/Latinos: A qualitative systematic review. American Journal of Preventive Medicine 33(5):418–427.
Rosenthal, E. L., J. N. Brownstein, C. H. Rush, G. R. Hirsch, A. M. Willaert, J. R. Scott, L. R. Holderby, and D. J. Fox. 2010. Community health workers: Part of the solution. Health Affairs 29(7):1338–1342.
Salazar, G., and M. B. Heyman. 2014. Benefits of attending a summer camp for children with inflammatory bowel disease. Journal of Pediatric Gastroenterology and Nutrition 59(1):33–38.
SCCC (Sickle Cell Community Consortium). n.d. Who we are. https://sicklecellconsortium.org/who-we-are (accessed January 15, 2020).
SCDAA (Sickle Cell Disease Association of America). 2019. Mission & vision. https://www.sicklecelldisease.org/mission (accessed January 15, 2020).
SCDAA. n.d. Grant project. http://sicklecelldisease.net/grant-project (accessed January 15, 2020).
SCDAAMI (Sickle Cell Disease Association of America, Michigan Chapter, Inc.). n.d. Home page. https://www.scdaami.org (accessed January 15, 2020).
SCDAI (Sickle Cell Disease Association of Illinois). n.d. About us. https://www.sicklecelldiseaseillinois.org/about_us (accessed January 15, 2020).
SCFGA (Sickle Cell Foundation of Georgia). 2018. Operations report 2018. Atlanta, GA: Sickle Cell Foundation of Georgia.
Scott, R. B. 1981. Whither sickle cell disease in the 1980s. Journal of the National Medical Association 73(4):307–308.
Shepanski, M. A., L. B. Hurd, K. Culton, J. E. Markowitz, P. Mamula, and R. N. Baldassano. 2005. Health-related quality of life improves in children and adolescents with inflammatory bowel disease after attending a camp sponsored by the Crohn’s and Colitis Foundation of America. Inflammatory Bowel Diseases 11(2):164–170.
Sickle Cell Association of Texas Marc Thomas Foundation. n.d. Home page. https://www.sicklecelltx.org (accessed January 15, 2020).
Sickle Cell Disease Foundation. n.d. MLK Jr. Outpatient Center for Adults with SCD. http://www.scdfc.org/scd-clinic-at-mlk.html (accessed January 15, 2020).
Skinner, M. W., J. M. Soucie, and K. McLaughlin. 2014. The National Haemophilia Program standards, evaluation and oversight systems in the United States of America. Blood Transfusion 12(Suppl 3):e542–e548.
Terry, M. 2018. A look at hemophilia drug prices and the market. BioSpace, July 3. https://www.biospace.com/article/a-look-at-hemophilia-drug-prices-and-the-market (accessed April 20, 2020).
Tozzi, J. 2015. This medical charity made $3.3 billion from a single pill. Bloomberg, July 7. https://www.Bloomberg.Com/news/features/2015-07-07/this-medical-charity-made-3-3-billion-from-a-single-pill (accessed April 20, 2020).
U.S. Pain Foundation. 2017. #makeitvisible movement raises awareness, funding for invisible illness. http://uspainfoundation.org/press-release/makeitvisible-movement-raises-awareness-funding-invisible-illness/#makeitvisible (accessed January 15, 2020).
WFH (World Federation of Hemophilia). 2020a. Country programs. https://www.wfh.org/en/our-work-reg-national/country-programs (accessed January 15, 2020).
WFH. 2020b. Over 50 years of advancing treatment for all. https://www.wfh.org/en/about/history (accessed January 15, 2020).
WFH. 2020c. Research and data collection. https://www.wfh.org/usa/programs/research-and-data-collection (accessed January 15, 2020).
WFH USA. 2018. WFH USA year-end report. Albany, NY: World Federation of Hemophilia.
WFH USA. 2020. Evidence-based advocacy. https://www.wfh.org/usa/programs/research-data-collection-evidence-based-advocacy (accessed January 15, 2020).
Wiltshire, J., K. Cronin, G. E. Sarto, and R. Brown. 2006. Self-advocacy during the medical encounter: Use of health information and racial/ethnic differences. Medical Care 44(2):100–109.
Wu, Y. P., J. McPhail, R. Mooney, A. Martiniuk, and M. D. Amylon. 2016. A multisite evaluation of summer camps for children with cancer and their siblings. Journal of Psychosocial Oncology 34(6):449–459.
This page intentionally left blank.












































